
Updated on June 24, 2025
Estimates from the Monthly Provision Study are updated, and become increasingly precise, as more data are collected over time. This update resulted in minor changes to estimates throughout the report and did not change any comparisons or conclusions.
New full-year estimates from Guttmacher Institute’s Monthly Abortion Provision Study show that the total number of abortions provided in all US states without total abortion bans remained relatively stable between 2023 and 2024, increasing by 1%, and the proportion of people traveling across state lines to obtain an abortion declined slightly, from 16% to 15%.
The overall stability in the number of abortions in states without total bans continued despite shifts in policy that have increased obstacles to accessing this care in many states. In 2024, 14 states* had total bans on abortion in effect, and Florida and Iowa implemented bans at six weeks’ gestation that drastically narrowed options for abortion access for both their own residents and (in the case of Florida) for residents across the region more broadly.
Accessing abortion services in the face of these obstacles—particularly for people residing in states with restrictive policies—has depended on a broad infrastructure of funding and navigational support. However, funding for this support network continues to be pushed to its limits, and the need for abortion services (and accompanying travel support for people residing in states with abortion bans) is unlikely to diminish.
What is included in our estimates?
The Monthly Abortion Provision Study estimates the number of clinician-provided abortions that take place each month in each US state without a total ban. It collects data on procedural and medication abortions provided at brick-and-mortar health facilities (such as clinics or doctor’s offices), as well as medication abortions provided via telehealth and online-only providers in the United States. Our estimates exclude any abortions provided in states with total bans (through shield law provision, community health networks, online pharmacies or other means), and therefore represent an underestimate of the total number of abortions nationally.
Changes in State-Level Abortion Provision in 2024
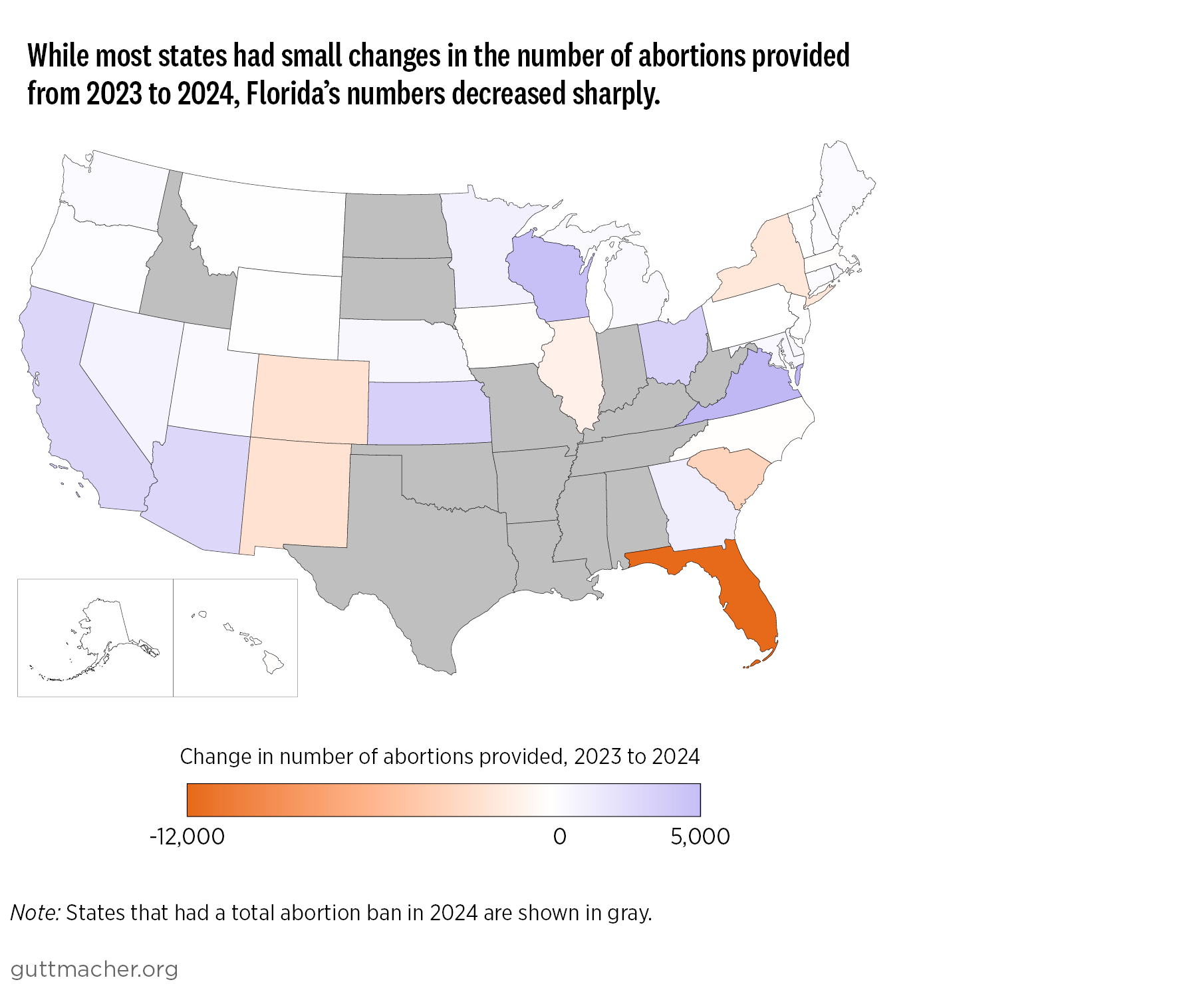
Despite a year characterized by large shifts in the abortion care landscape, the total number of abortions provided across all states without total bans stayed relatively steady in 2024 at 1,048,700, an increase of 1% from 2023 (Appendix Table 1). This stability at the national level masked substantial variability across individual states.
States with large decreases in abortions
- Florida experienced a particularly sharp decline in the number of abortions provided after a six-week ban went into effect in May 2024: Over the full calendar year, there were 11,200 fewer abortions provided in the state in 2024 than in 2023 (see map).
- South Carolina’s six-week ban went into effect in September 2023; as a result, the state had the second-largest decline (after Florida), with 2,700 fewer abortions provided in the state in 2024 than in 2023.
- Abortion totals in the protective states of Colorado and New Mexico declined by 2,300 and 2,600 cases, respectively, between 2023 and 2024, but total counts in these states remained substantially higher in 2024 than their baselines before Roe v. Wade was overturned in 2022.
States with large increases in abortions
- Clinician-provided abortion care was largely unavailable in Wisconsin following the overturning of Roe until the latter half of 2023; as a result, the state had a large increase from 1,300 abortions provided in 2023 to 6,500 in 2024 (an increase of 412%) as access expanded.
- Arizona, California, Georgia, Kansas, Ohio and Virginia had substantial increases in the number of abortions provided (ranging from an increase of 2,900 in Arizona to 6,600 in Virginia).
Increase in share of abortions provided by online-only clinics
The share of abortions in states without total bans that were provided via online-only clinics rose to 15% in 2024 from 10% in 2023 (an increase of around 50,000 abortions). Nationally, the share of abortions provided via online-only clinics is almost certainly higher than this, as the 15% proportion does not include shield law provision into states with total abortion bans. (Recent estimates from the #WeCount study document that 34,500 medication abortions were provided via shield laws to states with total bans in the first half of 2024.)
The increase in online-only abortion provision speaks to the critical role that these providers continue to play as abortion access in many states becomes more restricted. Where it is available, telehealth provision of abortion can significantly mitigate many of the barriers that patients face when seeking abortion services, such as lowering the costs and time needed to travel to a provider. Additionally, telehealth provision can sometimes reduce the stigma some people experience when seeking an abortion in person.
However, the majority of abortions in 2024 were still provided via brick-and-mortar facilities. Telehealth provision is not an available or preferred option for everyone seeking an abortion. At later gestational durations, for example, online medication abortion provision is often not an option, and people should be able to access the care they need using the method that works best for them.
Continued Travel Out of State for Abortion Care
In 2024, approximately 154,900 people crossed state lines for an abortion, representing 15% of all abortions provided in states without total bans (Appendix Table 1). This is a slight decline from 2023, when 169,900 people traveled across state lines for an abortion (16% of abortions in those states), but it is still close to double the number who did so before the end of Roe (81,100 in 2020). Travel to states with protective abortion policies remains a critical pathway for people seeking an abortion, particularly for those living in states with total bans or severe restrictions.
The states with the highest number of abortions provided to out-of-state residents in 2024 were the same four as in 2023:
- Illinois: 35,500 abortions, representing 39% of all abortions provided in the state
- North Carolina: 16,600 abortions (36% of abortions in the state)
- Kansas: 15,900 abortions (70% of abortions in the state)
- New Mexico: 12,700 abortions (69% of abortions in the state)
Illinois remains a key access point for the South and Midwest, because of both its geographic location and the efforts of the state government, abortion providers and support organizations to build a robust infrastructure to expand care and connect traveling patients with funding and navigational support. For example, two state government agencies have partnered with the Chicago Abortion Fund and several medical centers to ensure that abortion patients who need complex care in hospitals are supported. This program complements ongoing work in the state to help both Illinois residents and those coming from out of state seeking abortion care.
Kansas and Virginia saw substantial increases from 2023 to 2024 in the number of patients traveling from out of state: In Virginia, the number of out-of-state patients increased by around 4,400, and in Kansas, by 3,100. This increase in travel from other states was the main driver of increased abortion counts overall in both states, although other factors like expanded clinic capacity also may have increased access for state residents.
It is likely that Virginia absorbed patients affected by Florida’s six-week abortion ban after it went into effect in May 2024. Virginia is the second-closest state for Florida residents to seek an abortion after six weeks’ gestation (and the closest without a mandated waiting period); it may also be the most convenient option for residents of other states who previously would have traveled to Florida. Neighboring North Carolina instituted a 72-hour waiting period in mid-2023 that can make traveling to that state for an abortion difficult.
Out-of-state residents represented the majority of abortions provided in New Mexico in 2024 (69%), and one-quarter (25%) of abortions provided in Colorado. Both states, however, experienced declines in the overall number of abortions provided between 2023 and 2024, driven largely by declines in travel from out of state: New Mexico provided 2,000 fewer abortions to out-of-state residents in 2024, and Colorado provided 1,200 fewer.
The decreases in both states may be happening in part because of increases in clinic capacity in Kansas, which had an increase in abortions provided from 2023 to 2024. The decreases also may be related to broader access to medication abortion via shield law provision, which may allow some people (in states like Texas, for example) to access care remotely instead of traveling to New Mexico or Colorado. Both states saw particularly sharp drops in out-of-state abortion patients after July 2023, when some providers first started to offer telehealth provision to states with total abortion bans under the protection of shield laws in their home state. In addition, some of the decline possibly represents strains in the funding network for travel in the Southwest, as another sharp drop occurred in the last six months of 2024, a period during which funding for abortion support and care decreased (Appendix Table 2).
In all cases, travel across state lines can come at significant cost. People traveling from the South, in particular, often have to travel hundreds of miles and cross multiple states if they need or prefer to access in-person abortion services; they typically need lodging, childcare support and a variety of other services, in addition to the cost of the abortion itself. Obtaining abortion care out of state is often only possible because of the intensive efforts of providers, abortion funds, practical support organizations and patients themselves.
Continued Barriers to the Sustainability of Abortion Access
Residents of states with total or highly restrictive abortion bans continue to bear substantial burdens in order to obtain abortion services. Over the course of 2024, several states moved to protect abortion access; however, others continued to place tighter and tighter constraints on care. Several states, including some that have already banned abortion completely, have taken or are considering even further steps to prevent people from traveling to other states for care or to add to the growing threat of criminalization for pregnancy outcomes. A fundamental right to interstate travel is still protected nationally, including to leave a state with a total abortion ban to obtain an abortion in a state where care remains accessible.
Additionally, while patients, providers, abortion funds and practical support networks expend considerable effort to make abortion care accessible, they face an ever-increasing number of obstacles related to funding and capacity. These obstacles, coupled with the increasingly tighter legal and policy constraints on abortion provision, raise questions about the longer term sustainability of the funding and support landscape that has enabled many people to obtain an abortion, either in their own states or via travel to others.
Telehealth provision of abortion medication from providers based in states with shield laws to residents of states with total bans or restrictive policies likely continued to play a key role in maintaining access to care in 2024, particularly for those who do not want or need in-person care. However, shield law provision, like other efforts to improve abortion access, continues to face legal and policy attacks that seek to curtail legally protected services.
These increasing threats are further amplified by the national policy landscape. As states continue to introduce and pass new laws to further restrict abortion, the Trump administration has demonstrated its intention to decimate abortion access. Potential actions include enforcing a legally unsound interpretation of the Comstock Act in order to prohibit shipping abortion-related medication and medical equipment nationwide, implementing unnecessary regulations on telehealth provision of medication abortion through the US Food and Drug Administration, and imposing the “domestic gag rule” again to force reproductive health care providers to separate funds used for abortion-related activities and cease referrals for abortion services. Any of these policies, if acted upon, would push abortion care further out of reach for many people. In the coming years, the divide between the need for abortion and the ability for people to access it will only continue to expand.