Key Points
- The COVID-19 pandemic and its associated restrictions raised concerns that adolescents in Uganda may face barriers to receiving family planning commodities and services.
- Public and private service statistics data reveal that Uganda experienced smaller and shorter pandemic-related disruptions in adolescent access to sexual and reproductive health services than were initially anticipated.
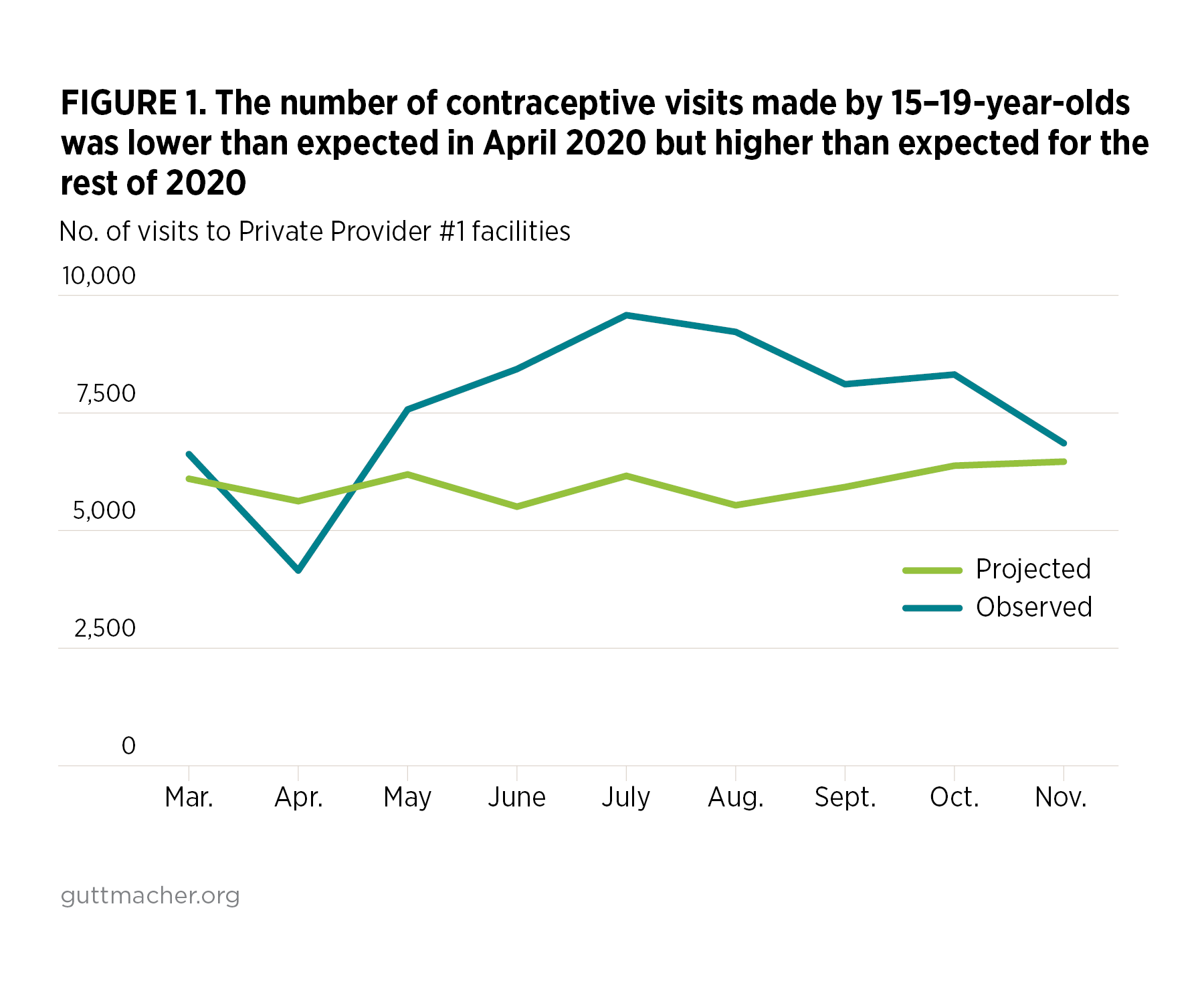
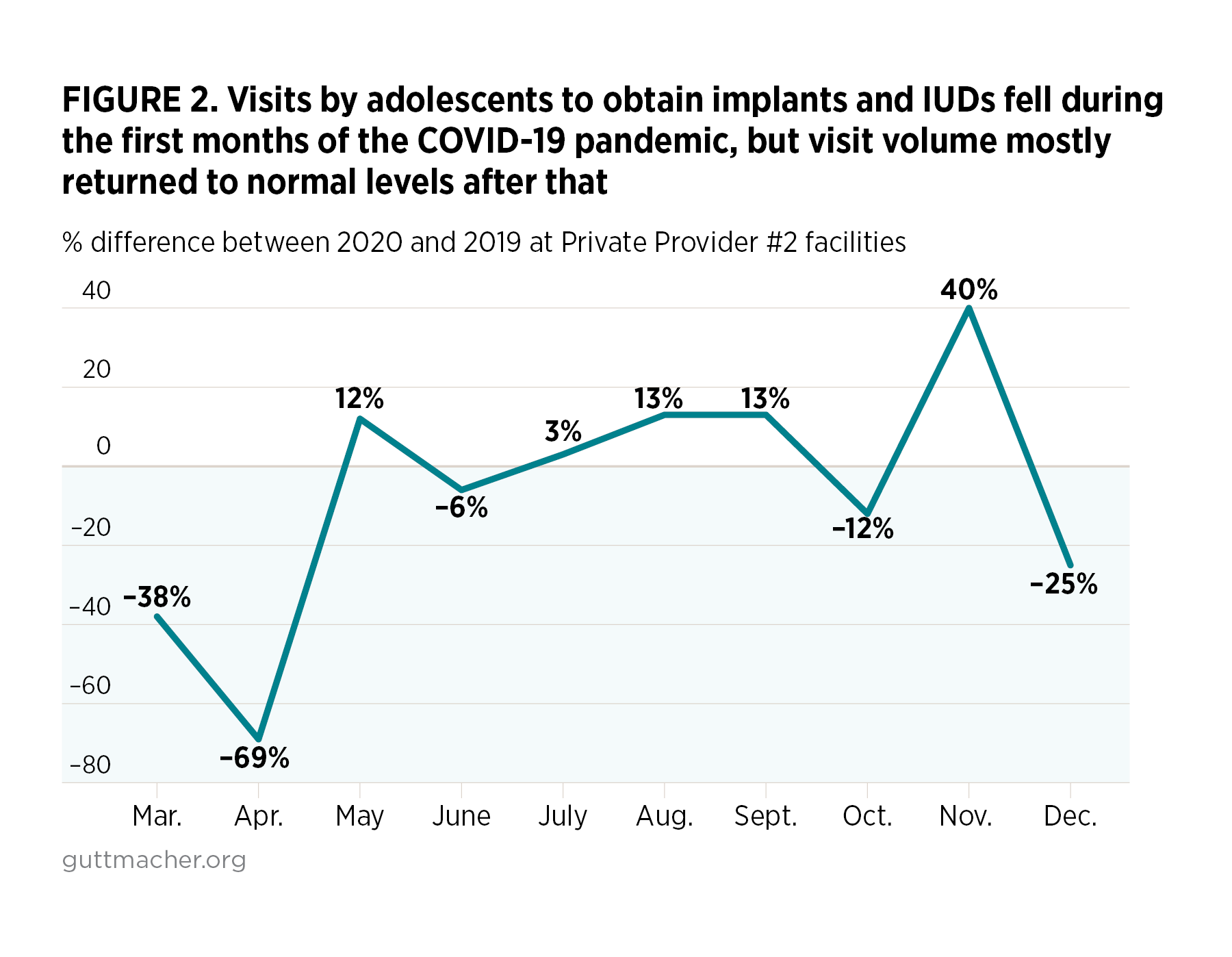
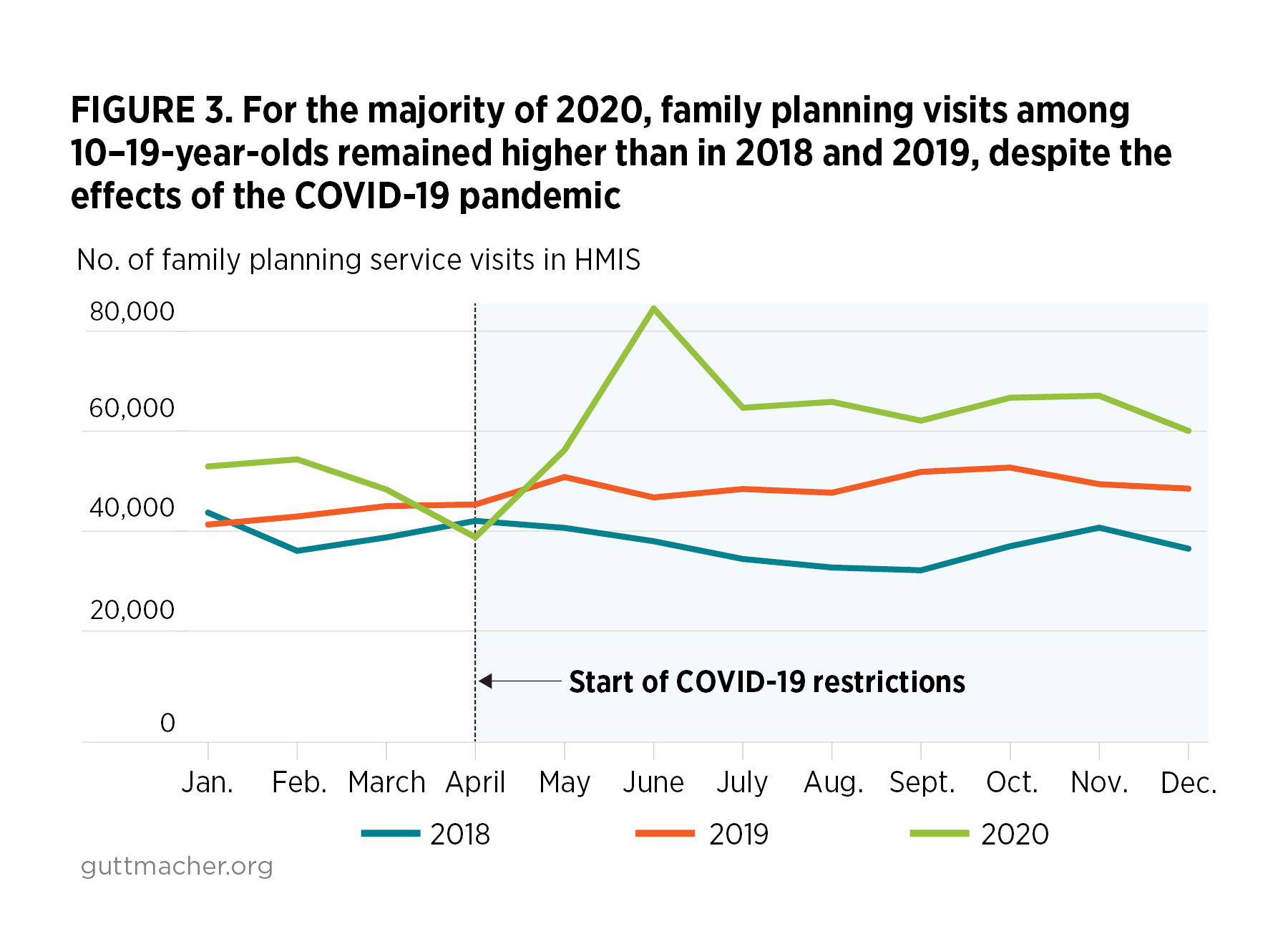
- A temporary dip in service visits during April 2020 was followed by a return to previous levels and even an increase in family planning visits among adolescent women during the remainder of 2020.
- These results speak to the resilience of the health system, which continued to provide services, and the impact of actions by partners to support access to reproductive health supplies and services.
- The Ministry of Health and other stakeholders should take the following steps to ensure adolescents’ continued access to sexual and reproductive health services throughout the remainder of the pandemic:
- Document and foster the adaptions and processes that helped ensure continuity of services during the COVID-19 restrictions, so that similar measures may be adopted in future crises.
- Promote meaningful participation of young people in COVID-19 task forces, to ensure that relevant policies are gender-inclusive and respond to young people’s sexual and reproductive health needs.
- Classify contraceptive care as an essential service, integrate it with COVID-19 response interventions and ensure that it remains fully operational and open before, during and after any future lockdowns.