
As a leading funder of global health programs, the United States has the power to make a tremendous impact on people’s sexual and reproductive health and rights. But restrictions on funding that target abortion care internationally have had broad, detrimental impacts on reproductive health care systems, advocacy and outcomes. Such is the case with the so-called global gag rule, a policy that conditions US global health assistance on nongovernmental organizations’ agreement not to provide or promote abortion.
Our multiyear research study in Uganda and Ethiopia examines the impact of this policy in two countries that rely on US assistance for their family planning programs but where the legal context around abortion differs—highly restrictive in Uganda and liberal in Ethiopia. Until now, no research has fully captured the effects of the most recent implementation of the global gag rule, which, during the four-year Trump administration, was the greatest expansion of the policy in its history. The research shows how, in both countries, the gag rule stalled and even reversed progress toward expanded access to modern contraception, impacting the countries’ reproductive health outcomes, the ability of people to decide whether and when to have children, and overall bodily autonomy.
Abortion care cannot be separated from reproductive health care; evidence clearly demonstrates that the US government’s attempts to limit abortion care through the gag rule also limit access to other essential sexual and reproductive health services. Although the gag rule is currently not in effect, the risk of an anti-abortion president reinstating and expanding the gag rule and causing significant harm to reproductive health progress globally remains. And even after the gag rule is rescinded, its effects persist. The time for a permanent end to the global gag rule is now.
What Is the Global Gag Rule?
The global gag rule is a policy, implemented through a presidential executive order, that deems non-US nongovernmental organizations (NGOs) ineligible for US government global health assistance if they provide, refer people for or promote abortion services—even if they use their own funding to do so. When the policy is in place, non-US NGOs that decide to continue receiving any US global health assistance must agree to stop providing or referring people for abortion-related services or advocating for the expansion of abortion access.
When the gag rule was conceived, in 1984,1 the 1973 Helms Amendment to the Foreign Assistance Act was already in place. The Helms Amendment prohibits the use of US funds to perform “abortions as a method of family planning” or to “motivate or coerce any person to practice abortions.”2 It applies to all US foreign assistance, including funding provided to US-based NGOs and foreign governments. The gag rule, which goes beyond Helms to target non-US funding, has been in place under every Republican president since Reagan and has been rescinded by every Democratic president, including President Biden in January 2021.3

When President Trump came into office, in 2017, he followed the precedent of Republican presidents before him and reinstated the rule. He also greatly expanded its scope. The Trump administration’s version of the gag rule was the Protecting Life in Global Health Assistance (PLGHA) policy.4 While prior iterations of the gag rule applied to only global family planning assistance, the Trump administration expanded the policy by applying it to all global health assistance. The Trump administration further expanded the gag rule two years later, in March 2019, by requiring recipients of US global health assistance to apply the rule’s restrictions to all of their non-US organization subgrantees in order to maintain their own eligibility for US assistance.5 These changes widened the reach of the global gag rule to a larger number of actors and further hurt global progress on reproductive health.
The Wide-Ranging Impact of the Global Gag Rule
For over two decades, researchers have documented varied harms associated with the gag rule, which include detrimental impacts on reproductive health advocacy, systems and services. Qualitative reports and studies of the Trump administration’s expanded gag rule, as well as earlier iterations of the policy, have revealed decreases in contraceptive services, clinic closures, discontinued mobile outreach services, loss of service integration, fractured partnerships and referral networks, and a weakened advocacy environment.6–9
The gag rule’s impact reaches beyond the organizations and activities that are subject to its restrictions. In theory, it targets only NGO programs and services, allowing ministries of health and public-sector programs and facilities to be exempt from the policy. However, in practice, it affects reproductive health services provided by NGOs via their affiliates and through public health systems. In many countries, NGOs that are subject to the policy provide a large amount of support to ministry of health programs. Thus, when NGOs decide not to comply with the gag rule and lose funding, those losses often get passed on to public-sector facilities and programs, impacting services across the entire health system.
Even when programs are not affected, the gag rule creates a chilling effect, whereby organizations are confused about what is permissible under the policy—such as care for complications of unsafe abortion10—leading to reluctance to engage in partnerships and programming that are related to abortion.
Furthermore, the gag rule is also likely ineffective at its stated goal; the policy may actually increase abortion, despite its theoretical intention to curtail abortion around the world. Quantitative research on the gag rule during the George W. Bush administration has shown how the policy was associated with increased rates of unintended pregnancy and abortion. One study found an overall decrease in contraceptive provision, reduced contraceptive use and increased rates of unintended pregnancy among rural women in Ghana.11 Other evidence suggests that abortion rates increased within countries affected by the gag rule when the policy was in place under President Bush and decreased when the policy was rescinded by the Obama administration.12,13
Compared with earlier versions of the policy, the expanded Trump administration gag rule affected more organizations and larger amounts of funding. It applied to all global health funding—approximately $12 billion—while earlier versions applied to around $600 million in family planning funding only.14 In addition, in 2019 the policy was extended to subcontractors of affected NGOs. New research was required to fully capture the impact of the expanded version of the policy.
To fill this gap, researchers at the Guttmacher Institute, alongside partners in Uganda and Ethiopia, examined how the policy affected health services and outcomes in the two countries. Both are heavily reliant on US global health assistance and represent two different legal contexts for abortion, enabling researchers to shed light on the impacts of the policy more broadly.
Uganda: Stalled Reproductive Health Progress
Uganda is a useful case study for learning about the impact of the gag rule. Historically, rates of modern contraceptive use in the country are low and unintended pregnancy and fertility rates are high, when compared with countries of similar economic status.15,16 Yet, in previous decades, Uganda saw steady increases in modern contraceptive use and decreases in the fertility rate.17,18 Community health workers (CHWs) have played a key role in more recent gains and are integral to providing community health care in Uganda.19–21 Most often recruited and trained by foreign NGOS, CHWs are organized and coordinated by the Ministry of Health. They have been found to be particularly effective in serving communities with limited resources and low use of modern contraceptives.22
Ugandans are particularly vulnerable to the impact of the gag rule because the US Agency for International Development (USAID) plays a major role in reproductive health services in the country and is by far the largest international donor to Uganda’s family planning budget.23 NGOs affected by the policy deliver more than half of Uganda’s family planning services,23 and they support public health facilities by providing commodities, training and mobile outreach visits.24,25
The Ugandan abortion law is highly restrictive, making abortion services unavailable for most people who need them.26 Because they were already functioning under those restrictions, some NGOs receiving US foreign assistance chose to comply with the gag rule. But two major NGOs serving millions of Ugandans annually refused to comply with the gag rule in order to honor their commitment to comprehensive reproductive health care and to advocating for safe abortion services. Their loss of funding eligibility caused a ripple effect that impacted much of Uganda’s family planning services.
The effect of the global gag rule
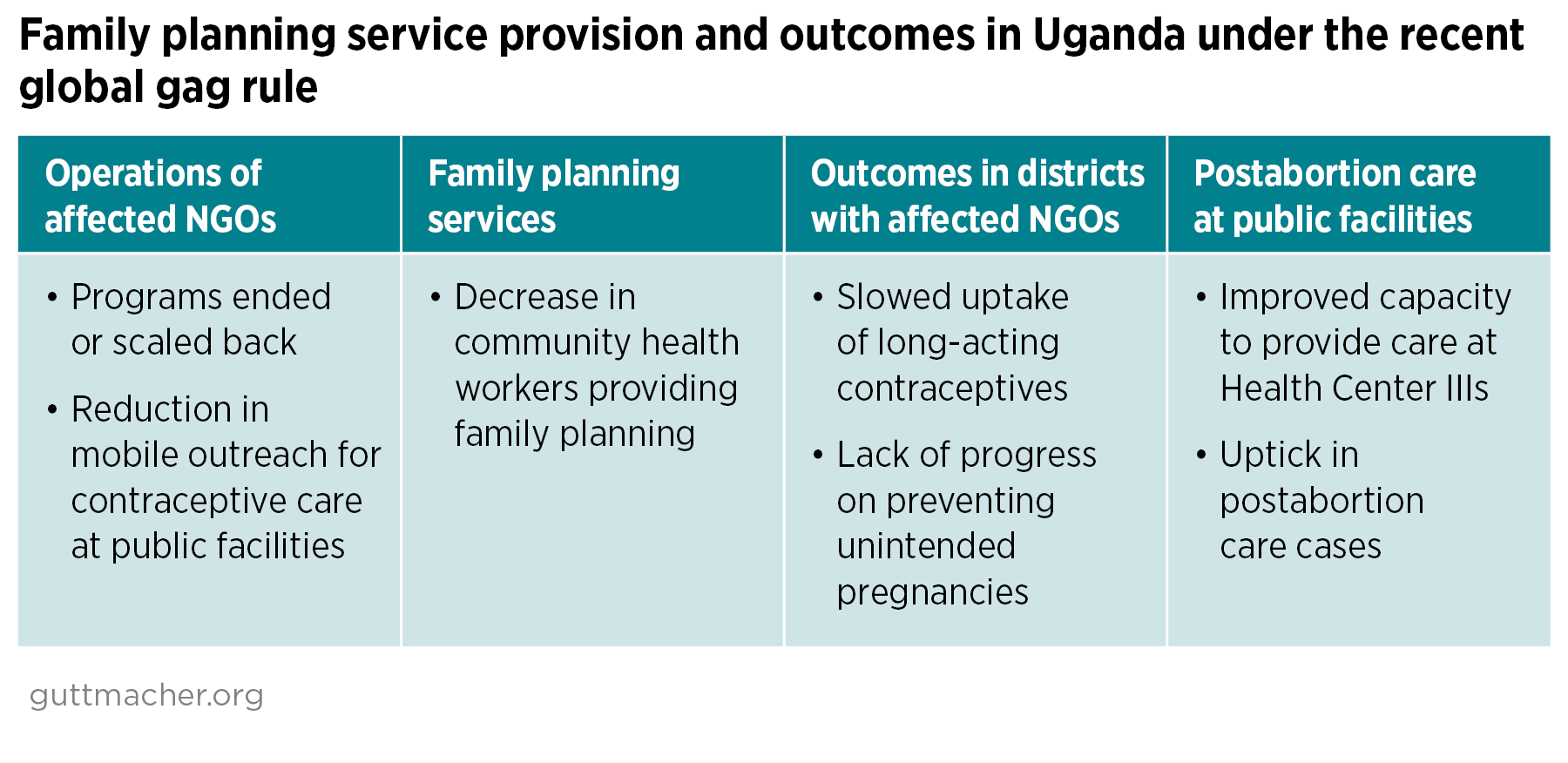
In the first year after enactment of the gag rule, researchers found that reproductive health outcomes differed among districts, depending on whether the NGOs affected by the policy had programs impacted in those areas. While people in districts where the policy had less reach continued to experience increased contraceptive use and decreased numbers of unplanned births, people in districts with more programs targeted by the gag rule failed to see such improvements.16 In districts where the policy had more reach, facilities engaged fewer CHWs to provide family planning services.27 Researchers posit that declines in CHWs’ community outreach to provide contraceptive education and counselling hindered women’s ability to correctly and consistently use contraceptives, harming progress that Uganda had made toward better reproductive health outcomes. In addition, the number of women in Uganda seeking postabortion care for complications from unsafe abortion increased during the period when the gag rule was in effect.28
In these ways, the gag rule stalled Uganda’s reproductive health progress, stagnating improvements in contraceptive use and potentially increasing rates of unsafe abortion. These harms will last well beyond President Biden’s revocation of the policy.
Ethiopia: Reversed Reproductive Health Progress
Ethiopia provides a good case study for investigating the effects of the gag rule. The country has made significant progress in improving reproductive health outcomes over the past 20 years and, in contrast to Uganda, represents a less-restrictive legal context for abortion.
In 2005, Ethiopia liberalized its abortion law. Since then, through government leadership and the work of NGOs, the availability of abortion care, contraceptive services and reproductive health outcomes have significantly improved. Over one decade, Ethiopia saw substantial decreases in maternal mortality due to unsafe abortion, while use of modern contraceptives more than doubled.29,30
Ethiopia has been able to make such strong progress in part through NGOs’ involvement in expanding reproductive health care through public sector services. NGOs have supported the Ministry of Health with mobile outreach programs that provide long-acting reversible contraception and by training public health workers, including health extension workers, who provide essential services to rural communities.6,31 In addition to the health extension workers employed by the public health system, community health volunteers have been instrumental to Ethiopia’s progress in improving reproductive health services.
Ethiopia is highly susceptible to the impact of the gag rule because it relies heavily on foreign donors—the United States, in particular—for family planning and reproductive health services. US global health assistance accounted for more than one-third of all development assistance for health received by Ethiopia in 2017.32 And funding from foreign donors, including the United States, has accounted for 70% of Ethiopia’s family planning budget.33
Many NGOs in Ethiopia complied with the terms of the Trump administration’s expanded gag rule to avoid losing US funding. But two large NGOs serving millions of people lost US assistance when they refused to comply with the gag rule’s restrictions.6 Because of this loss of funding, reproductive health services throughout the entire country faltered.

The effect of the global gag rule
Through an analysis of services before and after the global gag rule was enacted, researchers found countrywide declines in family planning services, including fewer facilities providing family planning through community health volunteers and mobile outreach.34 In addition, stock-outs of contraceptives increased. Because of the lost funding for the two large NGOs, a youth program reduced its geographic coverage, a mobile outreach program scaled back, a technical support program to the public sector ended and funding to sustain NGO operations halted.
The March 2019 expansion of the gag rule meant that regional development associations—parastatal organizations that conduct development activities—also had to comply with the rule. That compliance resulted in changes to services provided by these associations that were responsible for training health extension workers to, among other things, refer women for abortion care.34
Researchers also found a reduction in integrated services offering family planning and postabortion care after the gag rule went into effect.34 This finding is likely attributable to a chilling effect found in previous studies:10 NGOs are reluctant to provide postabortion care because of its proximity to abortion, even though postabortion care is permitted under the gag rule.
Despite the gag rule’s stated aim to limit abortion, concerted efforts by the Ethiopian government and NGOs that support the public health system ensured that abortion services were not harmed by the policy. While the gag rule was in effect, safe abortion services expanded in public health facilities; more safe abortions were provided and postabortion care cases declined.28 Unfortunately, the same cannot be said for other essential reproductive health services.
Overall, the gag rule disrupted the many years of progress that the country had made in improving the reproductive health of its population. This impact was particularly acute in areas where there were more service changes that resulted from the gag rule. In areas where the gag rule had less reach, increases in contraceptive use that had been seen prior to the policy stagnated.35 And in places with more exposure to the gag rule’s impact, contraceptive use decreased and births increased.
This reversal of trends toward improved reproductive health and increased contraceptive use will not be quickly remedied; it could take years to recover Ethiopia’s previous gains.
Recommendations for Policy Change
In January 2021, the Biden-Harris administration rescinded the global gag rule, but this alone will not repair the damage caused. The harm of the gag rule to reproductive health is far-reaching and long-lasting. Each time the gag rule is lifted, organizations can take years to restart interrupted services, regain funding, rebuild programs and partnerships and rehire staff.36 For example, organizations must wait for regular funding cycles to reapply for funding. All the while, reproductive health progress stalls. Without guidance from the US government, organizations may not fully understand what is and what is not allowable once the gag rule has been rescinded. Furthermore, the silencing of abortion information and advocacy under the gag rule can allow abortion stigma to proliferate and further embolden anti-abortion activists.
As a result of all these factors, the gag rule’s adverse effects remain well after it is withdrawn. Rescinding the policy via executive action alone is an insufficient solution; a permanent repeal of the gag rule is urgently needed. Several additional steps must be taken to support impacted organizations in rebuilding programs and services and to help meet the reproductive health care needs of people around the world.
Congress should pass the Global Health, Empowerment and Rights (Global HER) Act, which would permanently ensure that the gag rule cannot be reinstated.
The negative, lasting impact of the gag rule is clear. Across contrasting legal contexts for abortion, the policy erodes global progress toward improved reproductive health. The on-again, off-again nature of the policy creates uncertainty for US grantees as they try to plan programs and services. And the process of reinstating programs that were halted during the gag rule can take years as noncompliant organizations with multiyear contracts reapply for grants. Relying on Democratic administrations to repeatedly rescind the policy is not enough; the gag rule must be permanently repealed. By barring future presidents from reinstating the gag rule, the Global HER Act would accomplish this goal.
The Biden-Harris administration must issue clear guidance to implementing partners about what is allowable under current funding restrictions.
All agencies that administer global health programs, as well as US missions, must provide clear, ongoing and proactive communication to all past, current and potential partners about what it means for the delivery of sexual and reproductive health services when the global gag rule is not in place. One report suggests that, lacking clear and prompt guidance, organizations could not quickly readjust after the latest iteration of the gag rule was rescinded.36 There is a risk that US-funded organizations that complied with the gag rule will continue to avoid abortion work that was banned under the Trump administration or apply too restrictive an interpretation about what is allowed. In addition, the US government must ensure that all relevant training guidance, compliance guidelines, contracts, requests for proposal and related materials are up-to-date and reflect US support for sexual and reproductive health and rights.
The Biden-Harris administration must affirm the US commitment to global sexual and reproductive health, rights and justice.
With the overturning of Roe v. Wade through the Dobbs v. Jackson Women’s Health Organization decision, global perception that the United States is anti-abortion grew. It is incumbent upon the Biden-Harris administration to dispel this image and strengthen the United States’ leadership in sexual and reproductive rights internationally. The administration must integrate, promote and prioritize sexual and reproductive health, rights and justice across foreign policy priorities and global health, development and humanitarian programs. Not only would these steps embolden others in the global community to stand with the United States in support of these priorities, but they would also temper concerns about a US shift toward anti-abortion sentiment, which will remain unless the Biden-Harris administration consistently articulates strong, straightforward positions on these issues.
Congress should pass the Abortion is Health Care Everywhere Act to repeal the Helms Amendment.
The Helms Amendment has harmed individuals around the world for 50 years. Repealing the amendment would result in an estimated 19 million fewer unsafe abortions and 17,000 fewer maternal deaths each year if all abortions were made safe in countries where US foreign assistance is provided.37 Ending the Helms Amendment would also result in lower health systems costs by making more abortions safe and reducing costly abortion complications. Congress must pass the Abortion is Health Care Everywhere Act, which would amend the Foreign Assistance Act to repeal the Helms Amendment.
Repealing the draconian Helms Amendment and permanently repealing the global gag rule are inextricably linked. Both measures are necessary to allow US funds to support the full range of reproductive health services, including abortion care, around the world.