Key Points
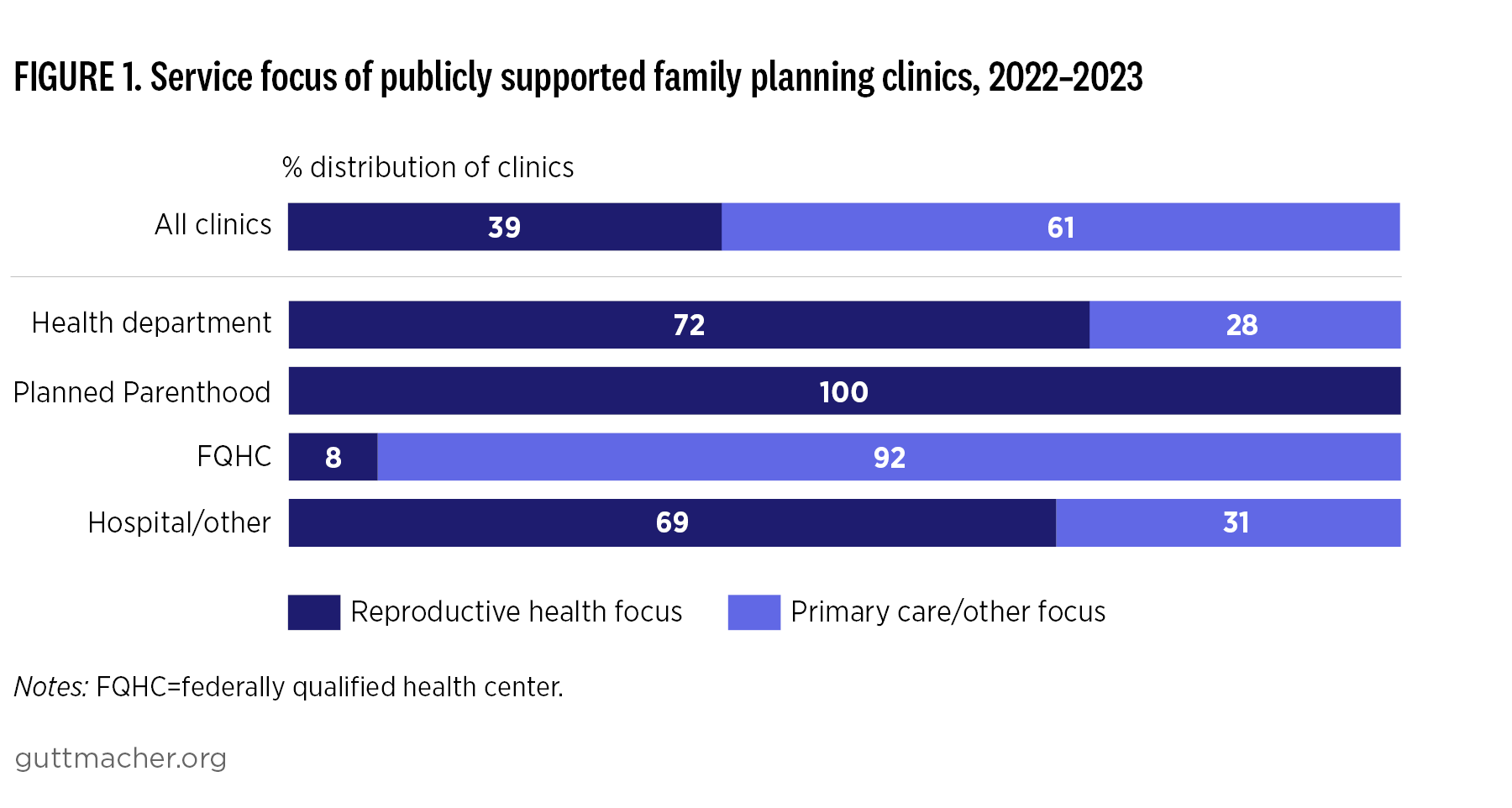
- Publicly supported family planning clinics play a crucial role in the health care system, providing essential contraceptive services to millions of people every year.
- These safety-net clinics have faced several obstacles since 2015, such as the Title X domestic gag rule, the COVID-19 pandemic and the overturning of Roe v. Wade.
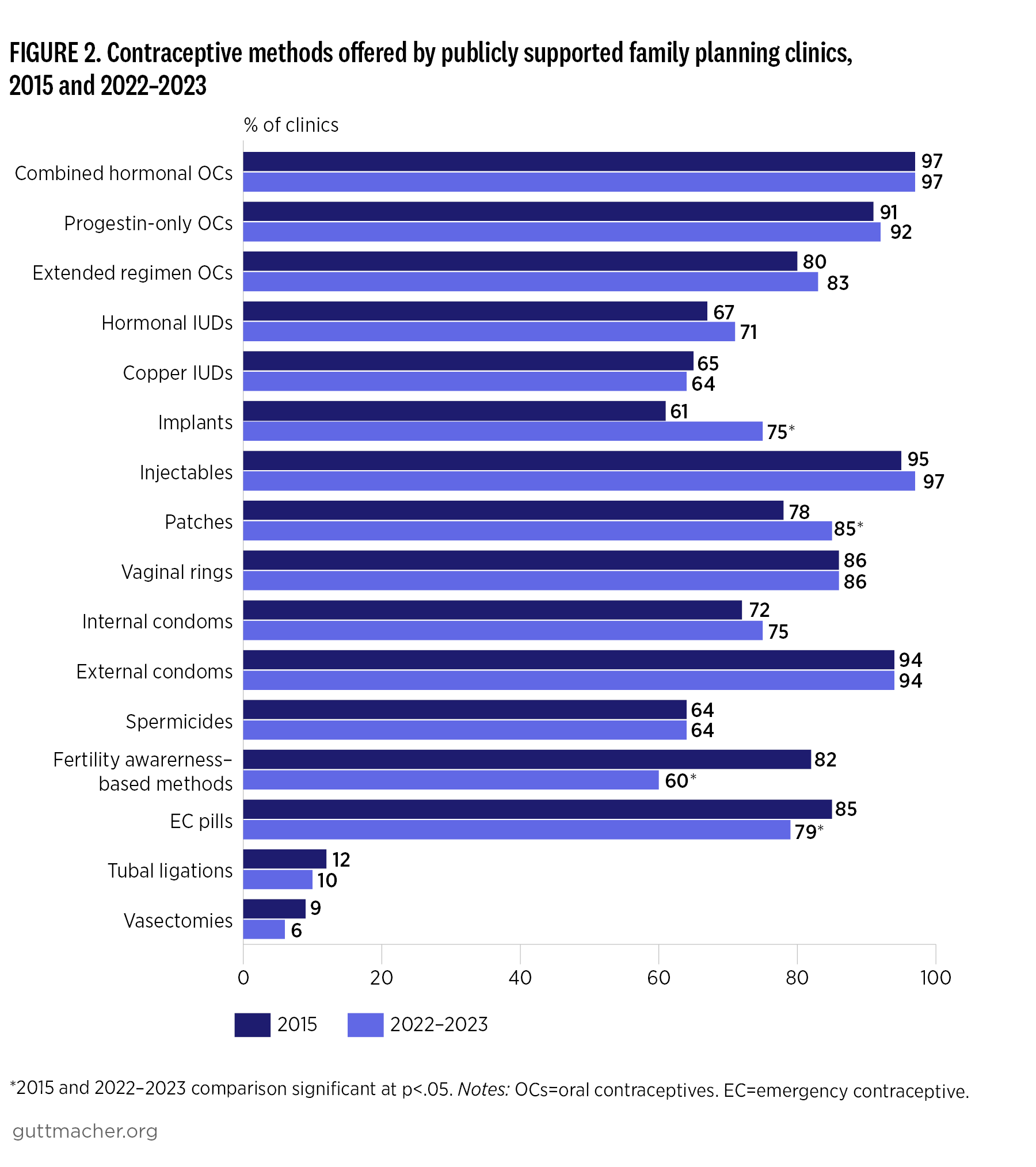
- The proportion of clinics offering a wide range of contraceptive services on-site has remained relatively stable since 2015. However, provision of implants has increased, while the number of clinics offering fertility awareness–based methods and emergency contraceptive pills has decreased.
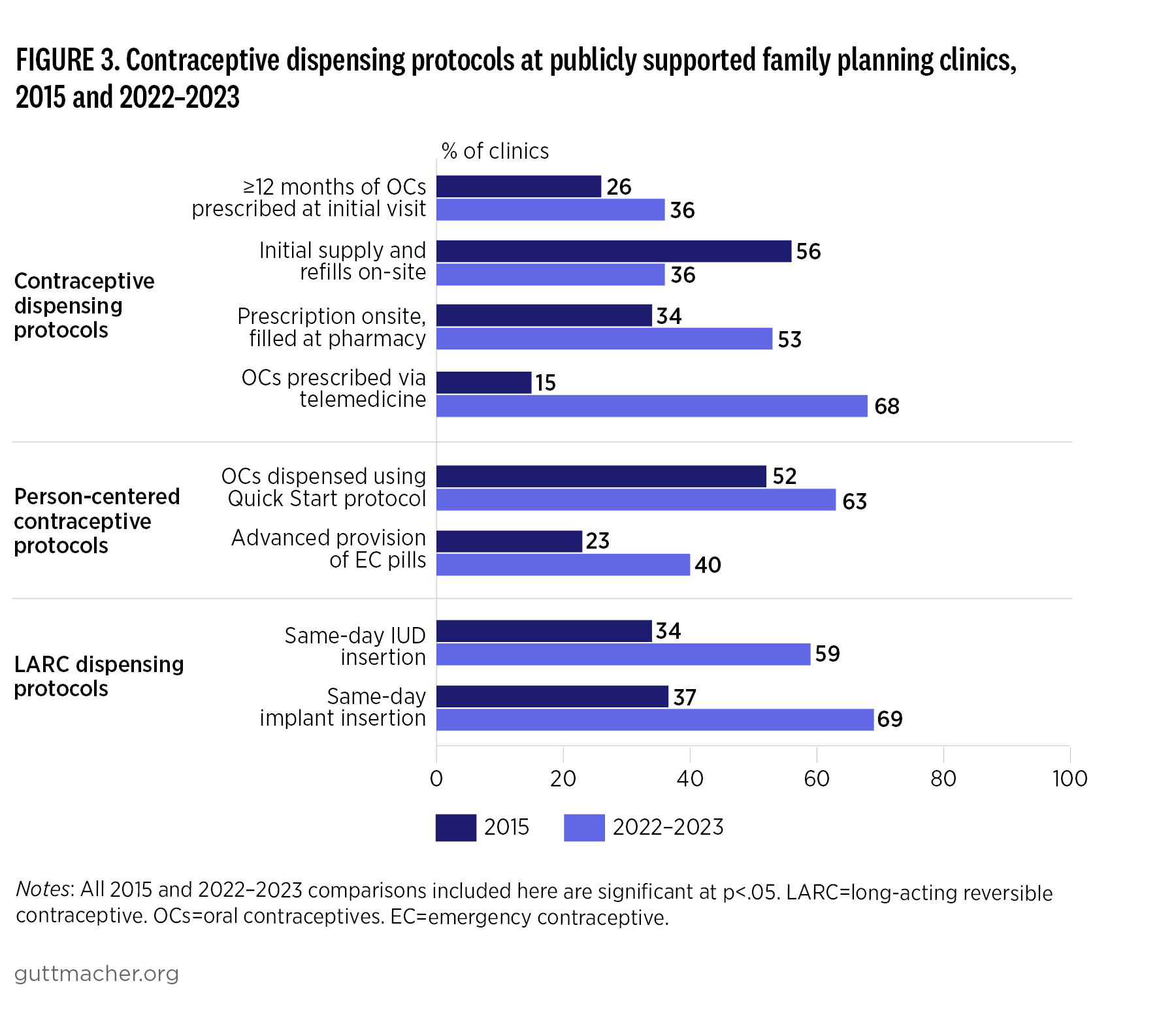
- The use of telemedicine to dispense oral contraceptive pills rose dramatically from 2015 to 2022–2023, likely driven by an increased use of telemedicine that began during the COVID-19 pandemic.
- The use of several protocols that support patient access to contraceptives has increased, including prescribing at least 12 months of oral contraceptive pills at the initial visit, offering both pills and refills on-site, dispensing oral contraceptive pills using the Quick Start protocol and offering advanced provision of emergency contraception, especially among Planned Parenthood clinics.
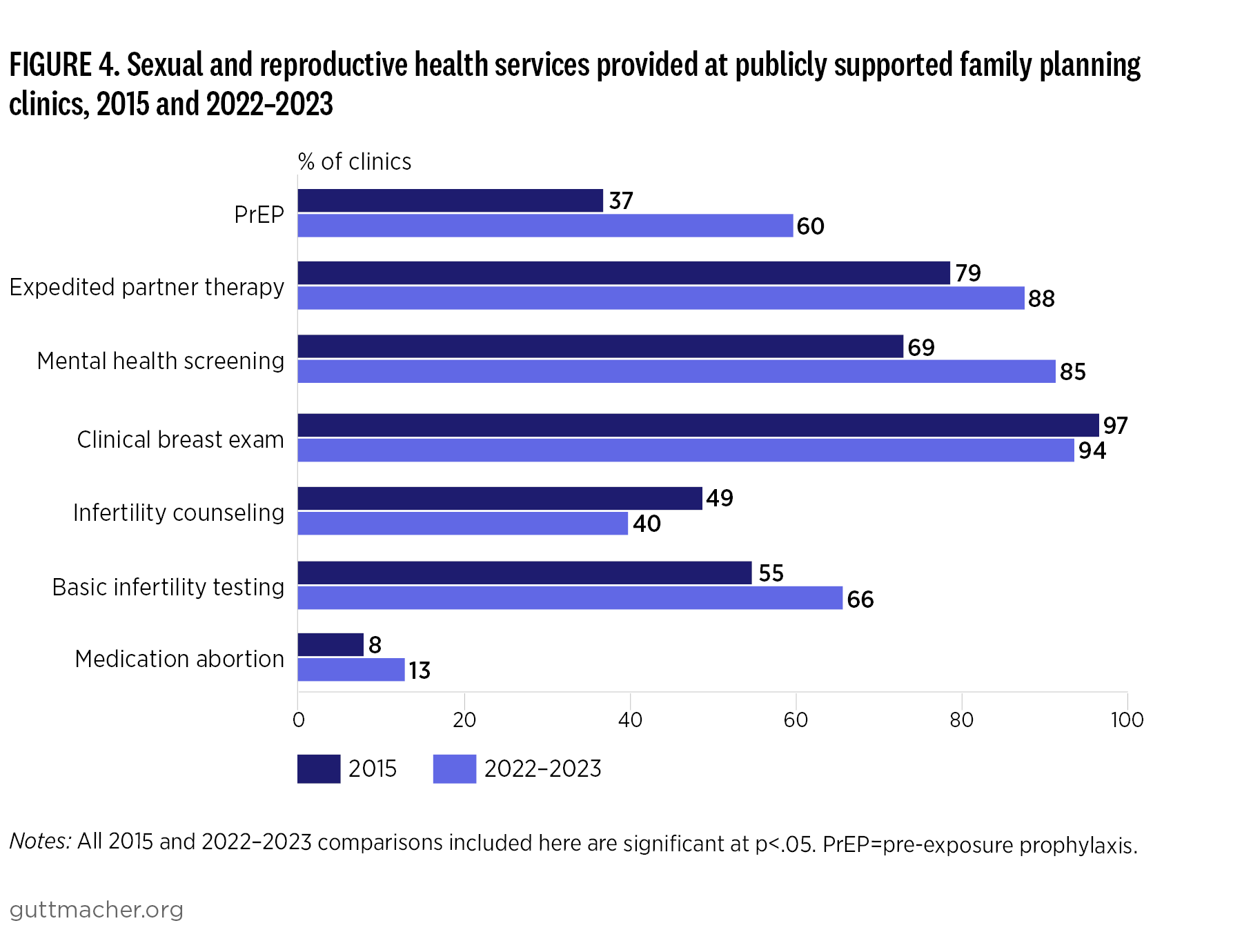
- The availability of general health and other sexual and reproductive health services in these clinics has also remained largely stable, although availability of HIV pre-exposure prophylaxis and mental health screening has increased notably since 2015.