

Title X, the United States’s publicly funded family planning program, was established in the 1970s with the express goal of reducing inequities in access to contraception and other reproductive health care. Because it helps clinics provide such services to people who have low incomes, are uninsured or come from disadvantaged communities, the Title X program is critical to ensuring reproductive autonomy.
The Title X program has long faced threats, including lawsuits and attempts to deny the program funding altogether. In 2019, the Trump-Pence administration imposed a harsh rule, known as the 2019 Title X Final Rule or “domestic gag rule,” prohibiting clinics that received Title X funds from providing patients with information and counseling about abortion. The policy caused many clinics to leave the Title X program and had devastating consequences for patients and providers. Though the Biden-Harris administration rescinded the 2019 Final Rule in 2021, the Title X program is still recovering, and other threats remain.
In the wake of the US Supreme Court’s Dobbs v. Jackson Women’s Health Organization decision revoking the constitutional right to abortion care, the landscape of sexual and reproductive health care in the United States is chaotic and fragile. Title X needs to be bolstered and fully funded; any further restrictions would cause even more turmoil for patients and providers than when the 2019 Final Rule was first implemented.
Impact of the 2019 Title X Final Rule
Implementation of the domestic gag rule undermined the ability of Title X to fulfill its core mission of ensuring access to a broad range of family planning services for millions of individuals with low incomes.
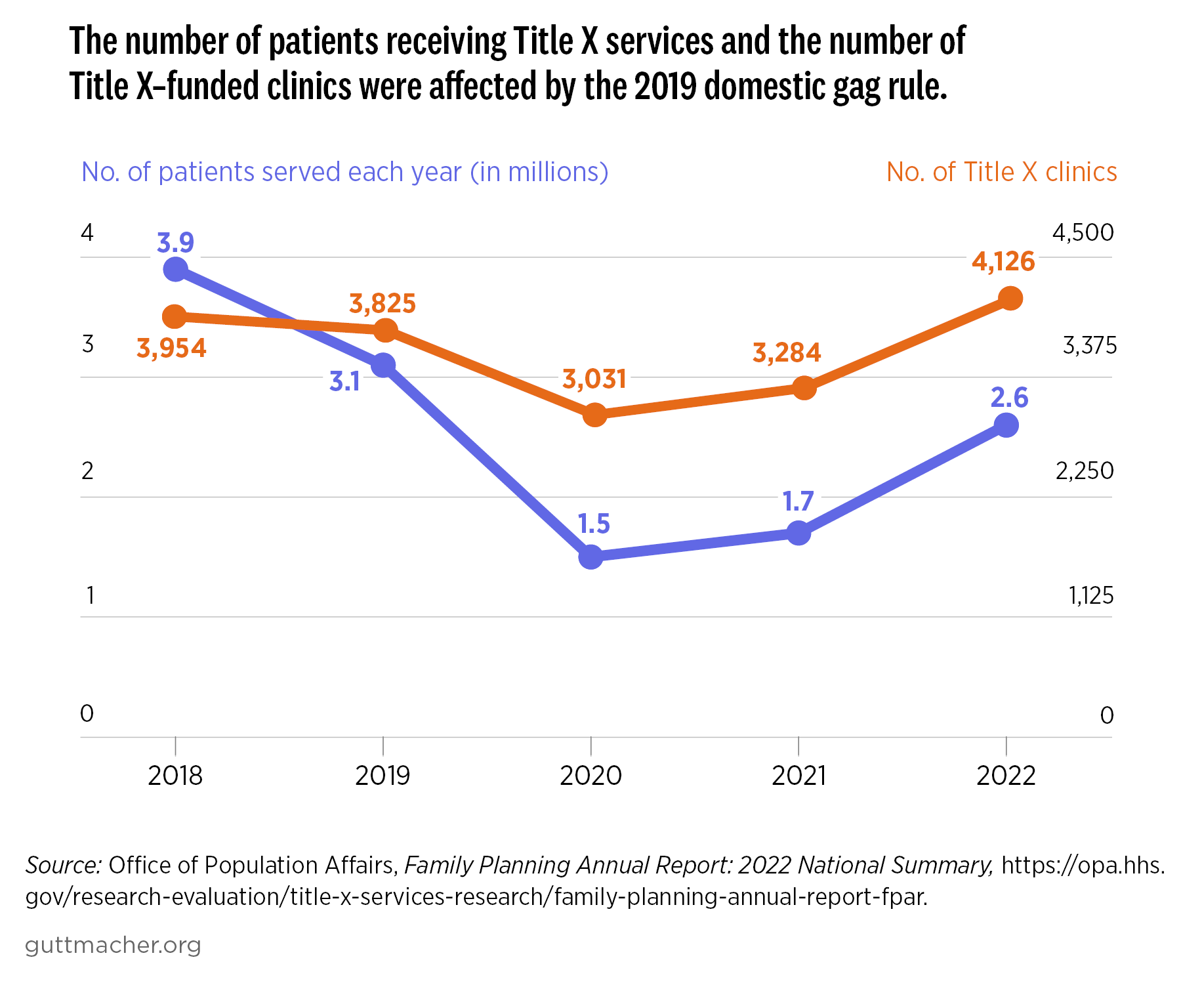
- In 2018, 3,954 clinics participated in the Title X program and 3.9 million people received Title X–supported services. In 2019 and 2020, those numbers dropped, before starting to edge back up in 2021.
- The number of patients served by Title X plummeted between 2019 and 2020, from 3.1 million to 1.5 million. Nearly two-thirds (63%) of that decrease is attributed to the 2019 Title X Final Rule and 37% to the impact of the COVID-19 pandemic.
- As a result of the domestic gag rule, six states (Hawaii, Maine, Oregon, Utah, Vermont and Washington) had no Title X clinics for nearly two years, and another 10 states had dramatic reductions in the number of available providers.
- Patients who originally sought family planning care at a Title X–funded clinic that subsequently left the program after the 2019 Final Rule were less likely to receive contraceptive care later on compared with patients who received care at a clinic that either did not leave the program or had not participated in it. Those who did receive contraceptive care from a clinic that left the program were less likely than those who received care at other clinics to use a method that requires interaction with a provider, such as an IUD, and to be satisfied with the method that they were using.
- Nearly eight in 10 clinics that left the Title X program following the 2019 Final Rule reported a decrease in funding from one or more sources, and these sites were more likely to change their sliding-fee structure or increase fees for some services, compared with sites that remained in the program.
- Clinics that stayed in the Title X program after the gag rule was imposed were less likely than those that left to provide comprehensive contraceptive and pregnancy options counseling.
Ongoing Challenges to the Title X Program
While the 2019 Final Rule was reversed in 2021, the network of service providers and clinics that receive Title X funds is still recovering from its negative impacts. Clinics faced substantial challenges following implementation of the domestic gag rule, including staffing changes and overhauling funding and payment structures, that were compounded by the COVID-19 pandemic. Reversing those changes after the rule was revoked in 2021 has been a costly, burdensome and protracted process for each clinic. Meanwhile, some clinics that left the Title X program have been slow to rejoin, and others have decided not to, particularly given the threat that new restrictions could be imposed based on who holds political power.
These disruptions deepened the Title X network’s ongoing struggle to meet the scope of need for publicly funded family planning services as a result of the program’s chronic underfunding. Title X has received approximately $286 million annually in funding from Congress—an amount that has not increased since 2015. That same year, government agencies estimated that Title X would need $737 million to serve women in need of the program’s services. More than eight years later, a tremendous need for increased funding remains, particularly in the wake of the destruction caused by the 2019 Title X Final Rule, the COVID-19 pandemic and inflation.
Today, Title X exists in a landscape in which access to reproductive health care is jeopardized, largely due to the wave of abortion restrictions following the Dobbs decision. A sizeable and growing body of evidence illustrates clearly how restrictions that may seem to target one type of reproductive health care have ripple effects on all aspects of reproductive health care, including contraception and pregnancy care. The 2019 domestic gag rule, which targeted abortion services and referrals, resulted in decreased patient use of their preferred contraceptive methods and had profound consequences for patients’ ability to access person-centered, quality care.
The ripple effect witnessed after the 2019 Title X Final Rule is also evident with the Dobbs ruling. Following the Dobbs decision, more women report trouble or delays accessing their preferred method of contraception, fewer women report receiving recent contraceptive care and fewer women report receiving person-centered contraceptive care. This is despite an increase in demand for such provider-involved methods as long-acting reversible contraceptives and sterilization methods for both men and women since the Dobbs ruling.
The Dobbs decision has exacerbated the same health inequities, including in access to contraceptive care, made worse by the 2019 domestic gag rule. The Title X program was designed to serve the populations most likely to face barriers to care. But the 2019 Final Rule contributed additional hurdles to care, including cost barriers, while also denying patients comprehensive counseling. Even before the domestic gag rule and the overturning of Roe v. Wade, Black and Hispanic women, women with low incomes and uninsured women were less likely to receive person-centered contraceptive counseling and more likely to face barriers to abortion care. Restrictions on Title X—whether those are reinstating the 2019 Final Rule or cutting funding, a recurring threat from anti-abortion members of Congress—would fall hardest on the communities already struggling the most with the fallout from the Supreme Court’s decision and deny individuals reproductive autonomy.
Title X–funded clinics are an important resource for patients seeking information about and referrals for abortion. Following the Dobbs decision, Title X grantees in some states must contend with state laws prohibiting options counseling that includes abortion information and referrals, which the federal program currently requires. New restrictions on Title X could prevent more participating clinics from providing this critical information, forcing patients to navigate even more hurdles to access abortion care.
Recommendations to Bolster Title X
The 2019 Title X Final Rule devastated the Title X program, harmed providers and threatened patients’ reproductive autonomy. Despite the rule being rescinded, the program has not fully recovered. Meanwhile, threats to the program have continued, and the country’s reproductive health care crisis has gotten worse. Rather than impose restrictions on Title X, we must invest in its success.
- Fully fund and strengthen Title X. Congress must ensure adequate funding for the program every year in annual appropriations legislation. In addition, lawmakers should ensure that Title X regulations are not subject to political intervention by any future administration aiming to undermine sexual and reproductive health and rights.
- Ensure that sexual and reproductive health care programs, including Title X, provide person-centered care. Providers must be able to give patients full information about their care and options, including comprehensive contraceptive options counseling and referrals for abortion care, without restrictions.
- Remove restrictions that silo abortion care in Title X and other sexual and reproductive health care programs. All forms of reproductive health care are inextricably linked. Restrictions on abortion and abortion stigma must be recognized as broader threats to sexual and reproductive health care.