Key Points
- Research in four states—Arizona, Iowa, New Jersey and Wisconsin—that have varying sexual and reproductive health policies illustrates that restrictions appearing to target one type of reproductive health care have ripple effects on all aspects of reproductive care, including abortion and contraception.
- Research on the Trump administration’s 2019 Title X Final Rule, also known as the “domestic gag rule,” and related state polices provides evidence that policies seemingly aimed only at abortion can negatively impact health care systems and provider delivery of sexual and reproductive health care, as well as patients’ experiences of person-centered care and reproductive autonomy.
- Living in a state where the policies are generally protective of sexual and reproductive health care does not necessarily insulate individuals from the impact of restrictive federal policies. For example, the number of clinics in the Title X network and the number of people served by those clinics declined in New Jersey after the domestic gag rule took effect, similar to declines seen in states with more restrictive policies, such as Iowa and Wisconsin.
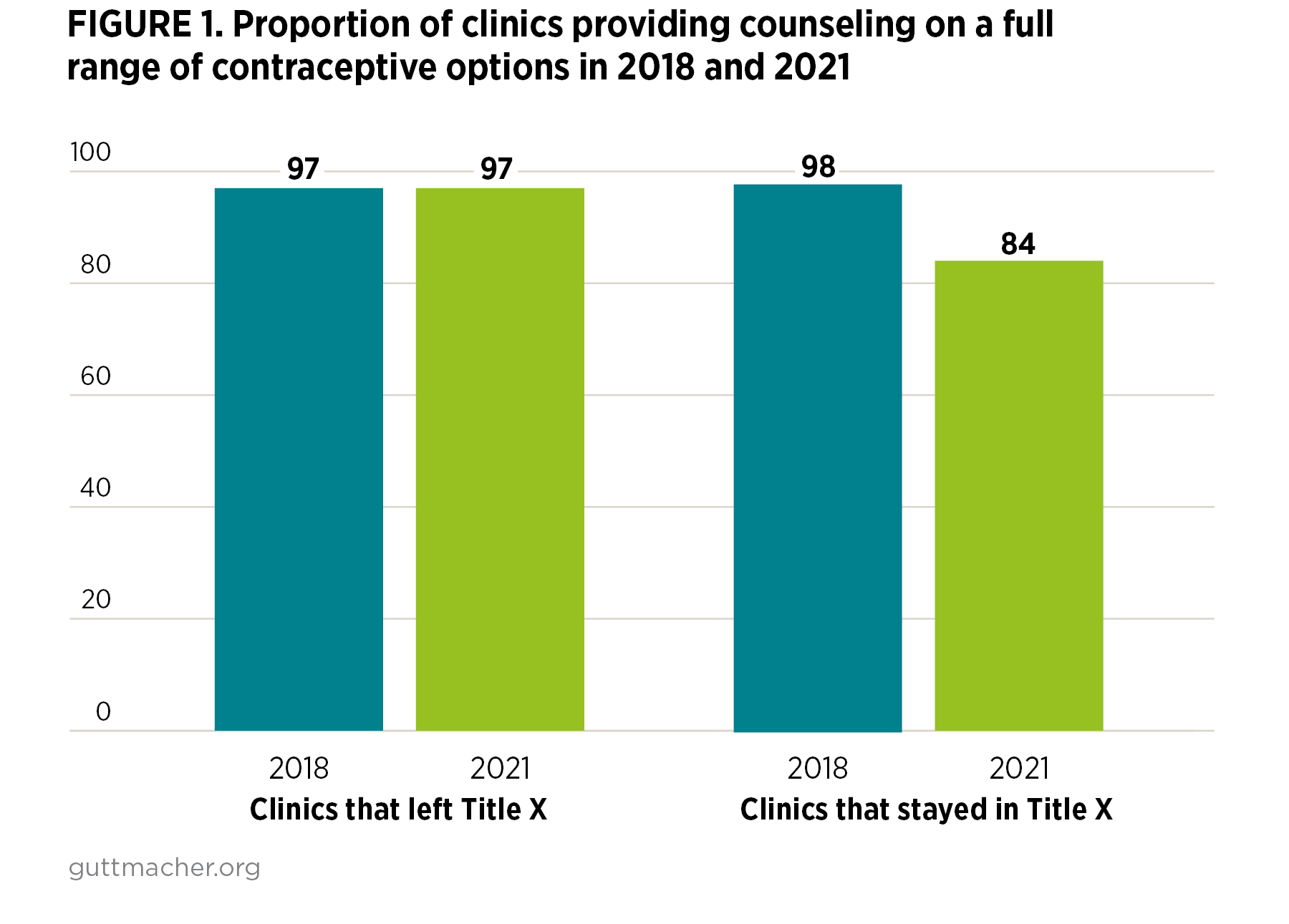
- The 2019 Title X Final Rule negatively impacted both clinics that chose to stay in and those that left the Title X network, limiting their services and the provision of person-centered care beyond what was dictated by the policy.
- Policy restrictions trickle down to impact individuals' experiences with care. For example, diminished access to high-quality, more affordable and more comprehensive sexual and reproductive health care resulted in some patients shifting their contraceptive use to a contraceptive method that they preferred less.
- Policy restrictions on sexual and reproductive health care compound existing inequities. Federal and state policies should fully fund Title X, ensure comprehensive coverage of all contraceptive options, and remove restrictions that silo abortion to promote reproductive autonomy and person-centered care.