In 2019, conservative state legislators raced to enact an unprecedented wave of bans on all, most or some abortions, and by the end of the year, 25 new abortion bans had been signed into law, primarily in the South and Midwest. Along with this new strategy, legislators also continued their efforts to adopt other types of abortion restrictions, including requirements for abortion providers to give patients misleading and inaccurate information about the potential to reverse a medication abortion as part of abortion counseling.
These state-level policy developments to ban or restrict abortion are also an important backdrop as the U.S. Supreme Court considers a Louisiana law in 2020 that requires abortion providers to have admitting privileges at a local hospital. The Louisiana law is identical to a Texas law the Court struck down in 2016, and reversing its own precedent only four years later would raise serious questions about the Court’s integrity and ability to respect settled law. A decision upholding the Louisiana law could also have a significant impact on those seeking abortion care in many parts of the country.
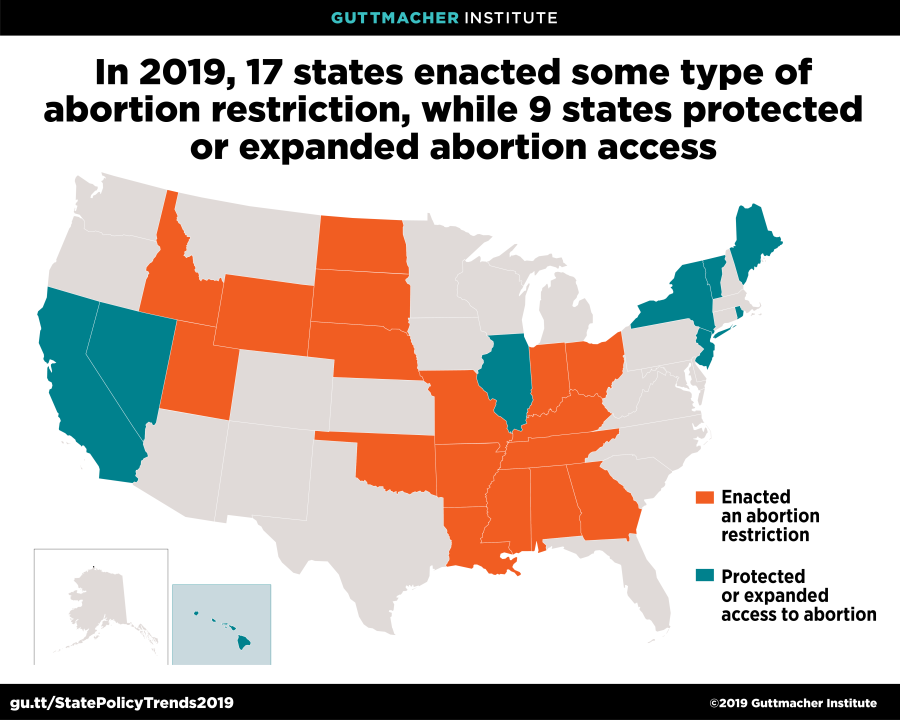
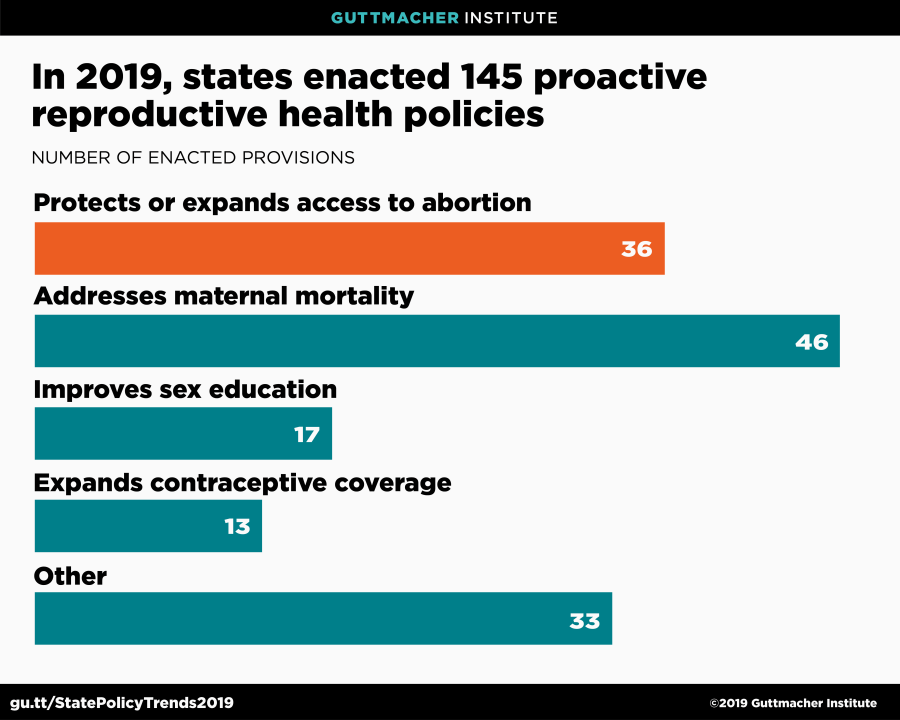
In direct response to efforts to undermine abortion access in other states and in the courts, state legislatures primarily in the Northeast and West, along with Illinois, are moving in the opposite direction. These legislatures have enacted policies that protect abortion rights and expand access to contraceptive services and sex education. This year, 36 measures that protect abortion have been enacted, along with 46 policies intended to decrease maternal mortality, 13 that increase access to contraceptive coverage and 17 that improve sex education. Also, governors in five states vetoed abortion restrictions. The new abortion protections are particularly notable: More were enacted this year than in the entire previous decade.
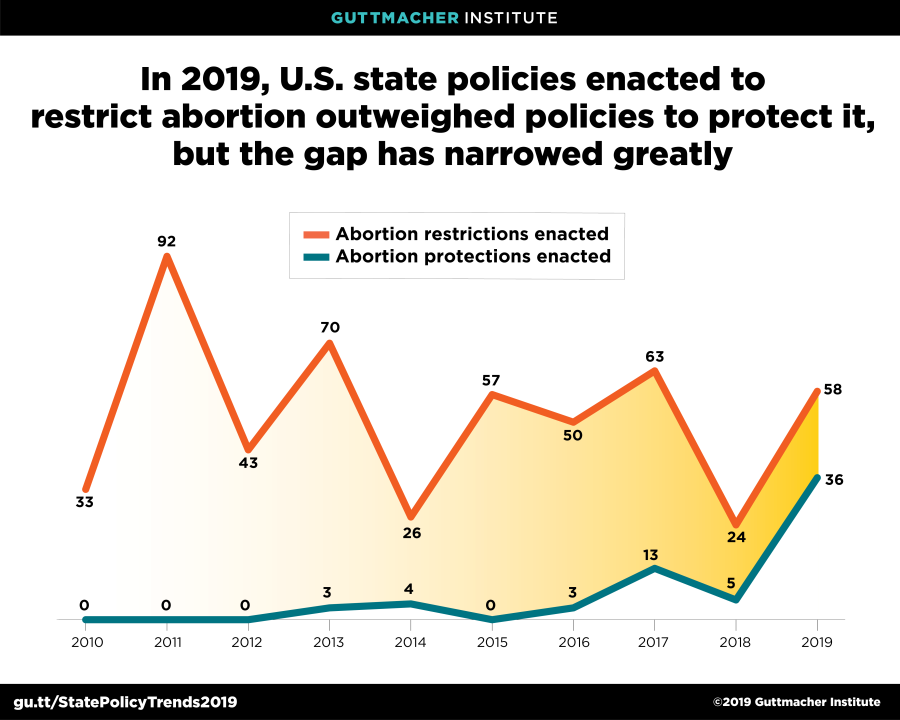
Nearly half of the 58 new abortion restrictions enacted in 2019 would ban all, most or some abortions. This surge in abortion bans is a distinct departure from the strategy deployed by abortion opponents for decades, which was to adopt less sweeping abortion restrictions with a cumulative impact of denying care to patients and forcing clinics to close. The latter approach had led to passage of laws that were less likely to be challenged in court than outright bans. By contrast, supporters of the new wave of abortion bans have made it clear that they are seeking to give the U.S. Supreme Court multiple opportunities to undermine or overturn long-standing constitutional protections for individuals seeking an abortion.
Abortion Bans
The 25 abortion bans enacted in 12 states in 2019 vary in scope, with some prohibiting abortion after a specific point in pregnancy, others prohibiting a specific method of abortion, and other bans hinging on the patient’s reason for seeking an abortion.
- Nine states enacted gestational age bans:
- Alabama enacted a total ban on abortion, at any point in pregnancy.
- Georgia, Kentucky, Louisiana, Mississippi and Ohio banned abortion when a fetal heartbeat can be detected, which could be interpreted to be as early as six weeks of pregnancy.
- Missouri banned abortion at eight weeks and included additional bans at three other gestational ages in anticipation of litigation over each ban’s constitutionality.
- Arkansas and Utah banned abortion at 18 weeks of pregnancy.
- In all of these states except Louisiana, lawsuits were filed to challenge the legislation and the bans are not currently in effect. In Louisiana, the law will not go into effect unless the Mississippi ban is upheld.
- Two states enacted bans on a specific method of abortion:
- Indiana and North Dakota banned the method that is the standard of care for surgical abortion after about 14 weeks of pregnancy.
- Enforcement of the Indiana ban has been blocked pending the outcome of litigation, while the North Dakota ban will not go into effect unless Roe v. Wade is overturned.
- Mississippi and West Virginia currently have a ban in place on this method of abortion.
- Four states enacted bans based on the patient’s reason for seeking an abortion:
- Arkansas, Kentucky, Missouri and Utah banned abortion of a fetus that has or may have Down syndrome.
- Kentucky and Missouri also banned abortion based on the race or predicted sex of the fetus, and Kentucky banned abortion for a diagnosis of a genetic anomaly.
- The bans in Arkansas and Kentucky have been blocked from going into effect during ongoing legal proceedings. The Utah ban will only go into effect if Roe v. Wade is overturned. The Missouri bans are in effect.
- Including the new Missouri bans, nine states currently ban abortion for purposes of sex selection. Two of those states also have a ban based on race selection, and two states have a ban in effect based on genetic anomaly.
- Four states (Arkansas, Kentucky, Missouri and Tennessee) adopted legislation that would ban abortion if the U.S. Supreme Court were to overturn Roe v. Wade.
- With these additions, eight states have "trigger bans" in place.
Abortion Counseling
Since 2015, several states have required that abortion counseling include information on the potential to stop the completion of a medication abortion after taking the first drug of the two-drug regimen—a claim that is not supported by credible scientific evidence.
In 2019, four states (Kentucky, Nebraska, North Dakota and Oklahoma) enacted this counseling requirement, and Arkansas amended an existing law that mandated this type of counseling. These laws require medical providers to inform patients about the potential to reverse a medication abortion as part of preabortion counseling and require that the state-provided counseling materials include this information.
- The Arkansas law amendment requires that medical providers give patients written information after taking the first drug, in addition to information conveyed in the preabortion counseling and the state materials.
- The newly enacted laws in North Dakota and Oklahoma have been challenged in court and their enforcement has been blocked pending the outcome of the litigation.
- With the addition of the new laws in Arkansas, Kentucky and Nebraska, six states now require information on "reversing" a medication abortion.
Abortion Protections
As legislators in other states attack abortion rights, progressive state legislators are responding to a more conservative U.S. Supreme Court by enacting protections and expanding availability. In 2019, nine states took major steps to protect or expand abortion access and governors in five states vetoed abortion restrictions passed by the state legislature.
- Four states enacted laws to affirm the right to abortion:
- Laws in Illinois, New York and Rhode Island protect abortion up to the point of fetal viability and when a patient’s life or health is at risk at any stage. Vermont’s law provides protections for abortion throughout pregnancy.
- All four laws also protect the right to contraception (including sterilization) and the right to carry a pregnancy to term.
- The Illinois, New York and Vermont laws prohibit interference in accessing services related to these rights and remove legal barriers to the provision of abortion by advanced physician assistants, certified nurse midwives and advanced practice nurses.
- With the addition of these four states, 13 states have statutory protections for abortion rights.
- New laws in Maine allow physician assistants and advanced practice nurses to provide abortion care and require Medicaid and private health insurance plans to cover abortion.
- California now requires student health centers on University of California and California State University campuses to provide medication abortion.
- Nevada repealed its unenforced criminal abortion statute, removing a legal mechanism for punishing abortion providers if Roe v. Wade were overturned.
- A New Jersey law protects the confidentiality of home addresses for employees and patients of reproductive health providers.
- New laws in Hawaii and New York prohibit employers from discriminating against employees or their dependents for their reproductive health decisions and use of reproductive health care services, including assisted reproductive technologies.
-
Governors in Kansas, Montana, North Carolina, Pennsylvania and Wisconsin vetoed a range of abortion restrictions.
- Montana’s governor vetoed a measure that would have prohibited abortion at 20 weeks postfertilization, which is 22 weeks after a woman’s last menstrual period.
- Measures that would have required a health care provider to preserve the life of a fetus delivered alive during an abortion procedure were vetoed in Montana, North Carolina and Wisconsin. (Existing prohibitions in Montana and Wisconsin remain in place.)
- The governors of Kansas and Wisconsin vetoed legislation that would have required abortion patients to receive counseling on the potential to reverse a medication abortion.
- The governors of Pennsylvania and Wisconsin vetoed measures that would have banned some abortions based on the patient’s reason for seeking the procedure. In Wisconsin, the governor vetoed legislation that would have banned abortion based on the race or sex of the fetus or because of a diagnosis or potential diagnosis of a genetic anomaly, including Down syndrome. In Pennsylvania, the governor vetoed a measure that would have banned abortion based on a diagnosis or potential diagnosis of Down syndrome.
- Montana’s governor vetoed legislation that would have required that patients are offered an ultrasound before obtaining an abortion.
Other Proactive Legislation
Beyond abortion, states have also enacted legislation that seeks to reduce maternal deaths and that protects and expands access to contraception and sex education.
Addressing Maternal Mortality
In recent years, state legislatures across the country have worked to address persistent racial disparities in maternal mortality: According to the Centers for Disease Control and Prevention, the maternal mortality ratio for black women is three times as high as the ratio for white women, meaning three times as many pregnancy-related deaths occur per 100,000 births.
In 2019, 22 states and the District of Columbia enacted new provisions to address this crisis. The efforts take two overall approaches to improving maternal health: 1) establishing or reviving lapsed statewide maternal mortality review commissions, and 2) expanding access to and improving the quality of maternal health services.
- Twelve states (Arkansas, Colorado, Idaho, Illinois, Minnesota, Nevada, New Mexico, New York, Ohio, Oklahoma, Rhode Island and Virginia) established maternal mortality review commissions.
- These panels are generally tasked with reviewing maternal deaths and providing recommendations to reduce maternal mortality in the future.
- The New York law establishes commissions for New York State and New York City.
- Another eight states (California, Georgia, Maryland, New Jersey, South Carolina, Texas, Washington and West Virginia) and DC enacted laws that support the work of existing commissions.
- The Maryland commission will now provide information and recommendations about maternal mortality to state agencies and local groups as a way to promote an integrated public health response; a related program will study and make recommendations to reduce disparities in maternal mortality rates, including social determinants related to maternal mortality.
- The new law in Texas requires collection of information on maternal care and postpartum depression, and evaluation of the use of telemedicine for pregnancy and postpartum care.
- New laws in 10 states (California, Colorado, Illinois, Indiana, Massachusetts, Minnesota, New Jersey, Texas, Virginia and West Virginia) aim to expand access to and improve the quality of health care to support positive maternal health outcomes.
- In four of these states, Medicaid will be expanded to provide additional services: Illinois will expand Medicaid coverage for pregnant women from 60 days postpartum to 12 months postpartum; New Jersey’s Medicaid will include doula services; Texas will require Medicaid to improve prenatal and postpartum care and require statewide initiatives to improve the quality of maternal health services and outcomes; and West Virginia’s Children’s Health Insurance Program will include pregnant women with incomes up to 300% of the federal poverty guidelines and the state Medicaid program will include pregnant women up to 185% of the guidelines.
- Four states (Colorado, Indiana, Minnesota and Virginia) expanded access to health care for pregnant patients who use substances through improved referral and funding for services.
Sex Education
State legislatures continue to focus on sex education, with legislation enacted in nine states (Arizona, Colorado, Connecticut, Illinois, New Jersey, New York, Tennessee, Utah and Virginia) and DC. State legislation passed this year primarily focused on expanding the scope of sex education to provide information on sexual consent, include LGBTQ students, and promote healthy and violence-free relationships. Including these new laws, 24 states and DC require some form of sex education.
- New laws in Illinois, New Jersey and DC require education on sexual consent:
- In Illinois, the instruction must include information on consent, withdrawal of consent and actions that do not constitute consent.
- The New Jersey law includes instruction on the right to refuse unwanted sexual activity and the importance of respecting others’ refusals.
- In DC, instruction must cover personal boundaries and healthy relationships.
- Four states passed laws related to education around sexual violence:
- Connecticut’s law requires education on prevention of sexual assault and dating violence.
- The New York law requires education on prevention of child sexual exploitation and abuse.
- Tennessee’s law encourages schools to provide age-appropriate sexual violence awareness education in grades 7–12.
- The Virginia law requires evidence-based and age-appropriate instruction on human trafficking.
- Arizona repealed a provision of the state’s sex education law that prohibited HIV/AIDS instruction provided to students in grades K–12 from offering positive information about homosexuality.
- Utah amended its sex education law so that schools may, but are not required to, include information on contraception.
- Colorado expanded requirements for sex education when it is provided in schools. The new law requires sex education to be provided without bias, expands the requirements for contraception education and adds requirements for providing information on adoption, abortion, parenting and infant abandonment. The curriculum must also cover recognition and withdrawal of sexual consent. In addition, the sex education material is not allowed to endorse a religion, use shame-based or stigmatizing language, use gender stereotypes or exclude LGBTQ individuals.
Insurance Coverage of Contraceptives
In 2019, four states with existing guarantees for contraceptive coverage strengthened and expanded those requirements. There are currently 29 states that have a contraceptive coverage guarantee.
- Amendments to New Mexico and New York laws require health insurance plans to cover, without cost sharing, all U.S. Food and Drug Administration–approved contraceptives, emergency contraception and sterilization.
- In both states, the amendments require private plans to cover over-the-counter contraceptive methods and require coverage for an extended supply of a method dispensed at one time—a six-month supply in New Mexico and a 12-month supply in New York.
- In New Mexico, coverage for male sterilization and male condoms was excluded from high-deductible private insurance plans (in order to comply with an interpretation of federal law around those types of plans).
- The laws also require both states’ Medicaid programs to cover up to a 12-month supply of contraceptives dispensed at one time.
Other Measures
A new Washington state law bars private health insurance plans, student health plans and Medicaid from automatically denying reproductive health care services based on a patient’s gender. The new law also requires coverage of condoms, services related to sexual assault, well-person preventive visits, prenatal vitamins and breast pumps.