New data from the Guttmacher Institute reaffirm that medication abortion is a fundamental component of abortion provision in states across the country, even as anti-abortion policymakers use all levers of government to target this safe and effective method of abortion care. For the first time, Guttmacher’s Monthly Abortion Provision Study includes state-level estimates of the proportion of abortions provided via medication in 2023 in states without total abortion bans. It also provides data on the proportion of abortions provided by online-only clinics in 2023 in states without total bans or bans on telemedicine provision.
As we learn more about how people access abortion care across the states in a post-Roe v. Wade environment, many policy attacks on medication abortion now target telemedicine provision or attempt to unnecessarily complicate the process of prescribing and dispensing medication abortion in person. And, despite clear medical evidence demonstrating the safety and efficacy of medication abortion obtained in-person or online, anti-abortion policymakers often ignore that evidence and promote false claims about risks.
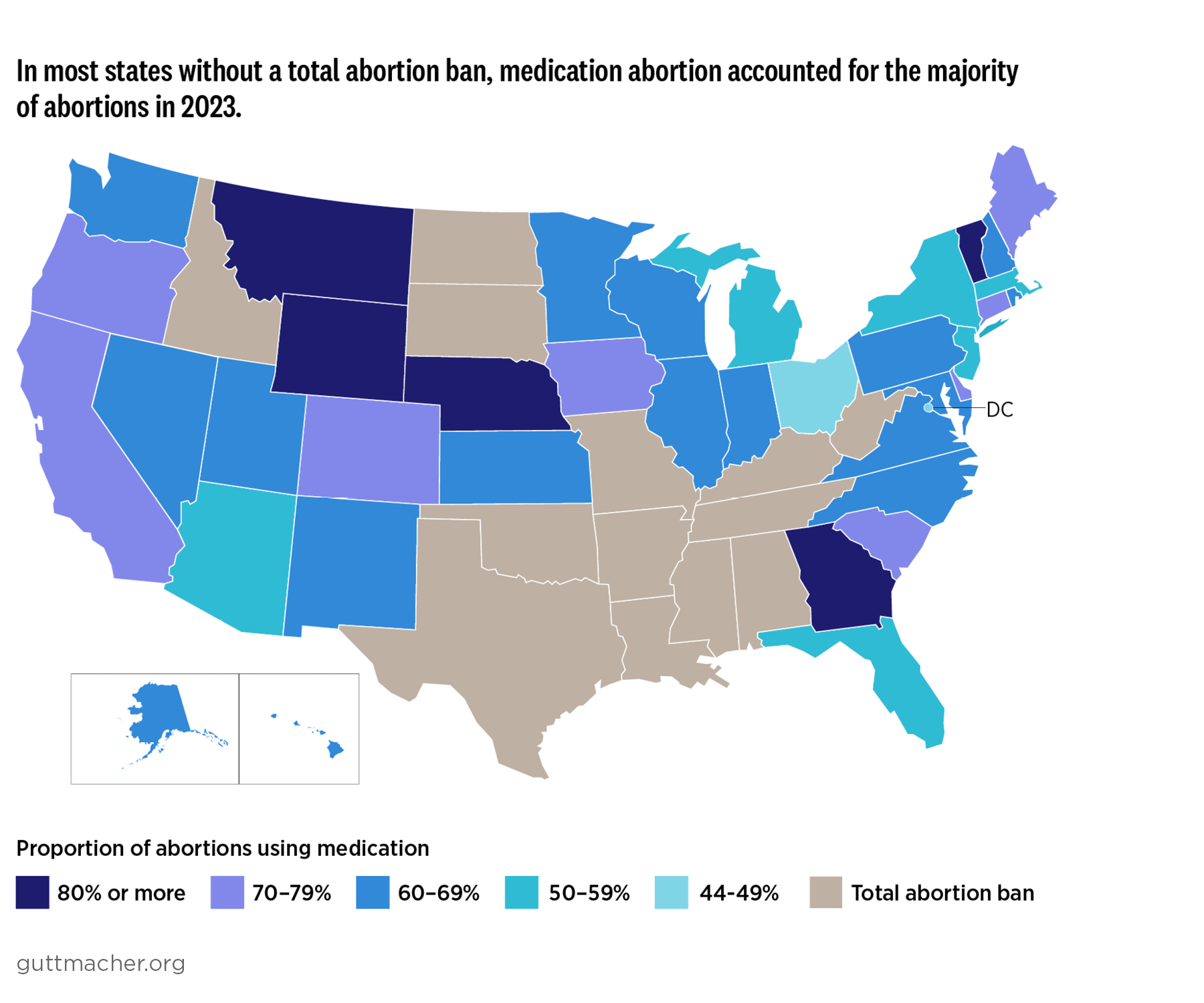
Latest Findings on Medication Abortion Provision by State
Per the most recent data, medication abortion accounts for the majority of abortions provided in most US states without total abortion bans. These results expand on Guttmacher’s finding that medication abortions accounted for 63% of all clinician-provided abortions in 2023 in states without total abortion bans. Proportions of medication abortion provision were lowest in the District of Columbia (44%) and Ohio (46%), and highest in Wyoming (95%) and Montana (84%; see table).
Medication abortion can be prescribed at an in-person clinic visit, or via telemedicine from a brick-and-mortar or online-only clinic. The new estimates indicate that one in 10 (10%) abortions in 2023 were provided by online-only clinics, with proportions ranging from 7% (California, DC and New York) to 60% (Wyoming).
The variation in proportions of medication abortion provision by state in Guttmacher’s estimates is not based on any single state characteristic. Rather, differences between states are likely related to interactions among a variety of state-level factors, including the number of abortion clinics and the proportion that offer medication abortion only, insurance reimbursement rates for abortion care, population density, telemedicine availability and the implementation of abortion policies.
Wyoming, for example, is a rural state with low population density, restrictive abortion policies and few abortion clinics, requiring many people to travel long distances for in-clinic care. The state has both the highest proportion of abortions provided via medication and by online-only clinics in 2023, indicating that many people may be avoiding the hardship of long-distance travel to a clinic by accessing services online. On the other hand, the proportion of abortions provided via medication was also high in Delaware, which has high population and clinic density as well as protective abortion policies. And the proportion was low in Ohio, a densely populated state with a mix of restrictive and protective abortion policies and relatively few abortion clinics for its size.
Data from the Monthly Abortion Provision Study do not include self-managed medication abortions (i.e., those not provided by a US clinician) or abortion pills mailed to people in states with total abortion bans. As a result, medication abortion likely plays an even more prominent role in the US abortion access landscape than the state figures presented here suggest.
Complex Factors That Influence Individual Choices
Medication abortion has become the primary method of abortion provision in most US states as it has become more accessible. A wide range of clinicians in many states are now able to prescribe it, and the US Food and Drug Administration (FDA) began allowing prescription via telemedicine in 2021. Furthermore, its use may be increasing as procedural abortion has become harder to access in many places following the 2022 US Supreme Court decision in Dobbs v. Jackson Women’s Health Organization.
Patients across the country are navigating a constellation of choices and constraints—around preferences, cost, availability, policy environment and geographic location—when they decide what type of abortion to have and where to have it. Differences in medication abortion proportions by state reflect a complex set of individual preferences and circumstances. Some people may opt for medication abortion because that option is available at the nearest or most accessible provider. Some choose medication via telemedicine because it is more affordable than in-clinic care or because they have limited ability to travel, take time off work or arrange child care. Others opt for medication abortion because they want to have their abortion in the comfort of their home or for other reasons. However, previous Guttmacher research suggests that some populations, including Black individuals and those with low incomes, are more likely to prefer procedural abortion to medication abortion. As a result, even though medication abortion accounts for the majority of abortions provided in most states, it may not be the preferred mode of care for everyone who uses this method.
National and State-Level Threats to Medication Abortion Access
The prevalence of medication abortion makes it a prime target of anti-abortion advocacy and lawmaking at the federal and state policy levels. These attacks often target access to mifepristone, one of two drugs used in the most common medication abortion regimen offered by US providers and approved for use starting in 2000. Decades of research have established that medication abortion using mifepristone is highly safe and effective.
And yet, anti-abortion activists have used misinformation and disinformation to advocate that the FDA rescind approval of mifepristone and reimpose restrictions that make it harder to prescribe. They have also advocated enforcement of the Comstock Act, antiquated federal legislation from the 1800s that they argue makes it unlawful to send medication abortion in the mail. With an anti-abortion majority in Congress and a second Trump administration that devalues reproductive health, bodily autonomy and evidence-based policies, threats to medication abortion may jeopardize access for all people, even those living in states where abortion is legal.
At the state level, anti-abortion lawmakers in several states have enacted legislation that limits the pool of providers by requiring that medication abortion be provided only by physicians. In addition, some states explicitly ban the provision of medication abortion via telemedicine or impose other restrictions, such as requiring an in-person visit for an initial exam, follow-up appointment or medication dispensing.
Increasingly, anti-abortion state legislators are pursuing novel legislative efforts to target medication abortion. Louisiana—which has a total abortion ban—was the first state to classify misoprostol and mifepristone as controlled substances in 2024, ignoring medical providers' concerns that the law would hinder their ability to treat life-threatening conditions. As of February 20, six other states have introduced similar bills in the current state legislative session. Other anti-abortion policymakers are seeking to subvert environmental laws to regulate medication abortion. These bills serve as models for policymakers around the country who seek to curtail or ban access to medication abortion. They also stigmatize medication abortion, attempting to undermine the drugs' high levels of efficacy and safety.
Attacks on Medication Abortion Through the Courts
Anti-abortion state lawmakers and advocates are not limiting their tactics to legislative action. In January 2025, Judge Kacsmaryk of the Northern District federal court in Texas ruled that the states of Missouri, Kansas and Idaho could move forward with a lawsuit to force the FDA to reinstate outdated restrictions on mifepristone. Focusing on individual providers is another route: A Texas civil lawsuit and a Louisiana criminal suit have been filed against a New York doctor for providing medication abortion to individuals in these two states. These are the first lawsuits in the country to challenge protections for abortion providers under a state’s shield law. These efforts to use the judicial system to restrict access to abortion will create a chilling effect among providers and may deter providers and patients from providing and seeking the care they need.
Conclusion
Monthly Abortion Provision Study data make clear that medication abortion is an essential option for people across the country, even as both the federal and state landscapes become increasingly hostile and difficult for providers, patients and those helping abortion seekers. State-level differences in medication abortion provision highlight the complex interplay between state characteristics and the unique circumstances that every person must navigate to access abortion care. Lawmakers at all levels of government should repeal medically unnecessary restrictions on abortion and pursue solutions that protect and expand people’s access to their preferred method of abortion care with safety and dignity.
Methodology
Data on medication abortion and online-only provision for 2023 are from Guttmacher’s Monthly Abortion Provision Study, which produces estimates of the number of abortions provided by clinicians in states without total abortion bans based on data collected from samples of abortion providers. Questions about medication abortion were included in versions of the survey distributed to providers in August and September 2023 and in February 2024 (with the latter asking providers for annual medication abortion figures for 2023). Estimates include abortions provided at brick-and-mortar facilities (including those that use telehealth) and online-only providers. These estimates do not include self-managed abortions or any abortions involving medication mailed to states with total abortion bans (either self-managed or provided by out-of-state clinicians).
Proportion of abortions provided via medication and by online-only clinics in US states without total abortion bans, 2023 | ||
| State | Proportion of abortions provided via medication (90% uncertainty interval) | Proportion of abortions provided by online-only clinics (90% uncertainty interval) |
| Alaska | 66% | † |
| Arizona | 59% (57–61%) | † |
| California | 71% (70–71%) | 7% (7–8%) |
| Colorado | 72% (69–74%) | 22% (21–23%) |
| Connecticut | 72% (71–72%) | 11% |
| District of Columbia | 44% (43–46%) | 7% (6–8%) |
| Delaware | 77% | 28% (27–28%) |
| Florida | 55% (53–57%) | † |
| Georgia | 83% (81–85%) | † |
| Hawaii | 66% (65–66%) | 12% (12–13%) |
| Iowa | 76% (75–77%) | 29% (28–29%) |
| Illinois | 60% (59–62%) | 10% |
| Indiana‡ | 63% | † |
| Kansas | 65% (64–65%) | 9% |
| Massachusetts | 57% (55–59%) | 12% (12–13%) |
| Maryland | 67% (64–69%) | 12% (11–12%) |
| Maine | 70% (68–73%) | 20% (19–20%) |
| Michigan | 58% (56–60%) | 9% |
| Minnesota | 63% (61–65%) | 21% (20–22%) |
| Montana | 84% | 16% (14–18%) |
| North Carolina | 61% (60–63%) | † |
| Nebraska | 83% (82–83%) | † |
| New Hampshire | 68% (66–71%) | 16% (15–17%) |
| New Jersey | 57% (54–60%) | 9% (8–10%) |
| New Mexico | 63% (62–64%) | 9% |
| Nevada | 69% (65–73%) | 24% (23–24%) |
| New York | 58% (57–60%) | 7% |
| Ohio | 46% (44–49%) | † |
| Oregon | 70% (69–71%) | 9% (8–9%) |
| Pennsylvania | 61% (60–64%) | 8% |
| Rhode Island | 60% (60–61%) | 18% |
| South Carolina | 74% | † |
| Utah | 60% (58–62%) | † |
| Virginia | 66% (63–68%) | 20% (19–22%) |
| Vermont | 81% (80–81%) | 12% |
| Washington | 66% (65–68%) | 15% (15–16%) |
| Wisconsin | 63% | † |
| Wyoming | 95% (91–98%) | 60% (48–66%) |
†Data unavailable; state banned the use of telemedicine for medication abortion provision in all or part of the year. ‡Data for Indiana include only abortions provided before August 2023, when a total ban took effect in the state.
Note: Some proportions are not associated with an uncertainty interval, either because data were obtained from all known providers in a state or the upper and lower bounds of the interval round to the median value.
Suggested citation: Friedrich-Karnik A, DoCampo I and Gibson C, Medication abortion remains critical to state abortion provision as attacks on access persist, Policy Analysis, New York: Guttmacher Institute, 2025, https://www.guttmacher.org/2025/02/medication-abortion-remains-critical-state-abortion-provision-attacks-access-persist.