In 2024, the US sexual and reproductive health and rights (SRHR) landscape remained deeply fragmented. Many states enacted policies to expand access to sexual and reproductive health services, including state constitutional protections for abortion that passed by ballot initiative in seven states. But other states started or continued enforcing draconian abortion bans and other restrictions that limit people’s bodily autonomy and aim to instill fear around seeking abortion care.
With an incoming Trump-Vance administration in 2025, this divide between protective and restrictive states may widen: Protective states may find innovative ways to support sexual and reproductive health care and rights, while restrictive states may double down, emboldened by a hostile administration. Moreover, new federal policies, such as additional restrictions on medication abortion pills or even a national abortion ban, could impact everyone, regardless of what state they live in.
In this year's state trends analysis, we will examine the state policies that laid the groundwork for these national dynamics. This year, we are also including statements from partner organizations across the United States who are working to safeguard reproductive health and rights. Their perspectives highlight how state policies impact grassroots organizations and the communities they serve.
Counts of State Legislation in 2024 (as of December 13, 2024)
Sexual and reproductive health and rights overall
2,458 provisions introduced that would protect sexual and reproductive rights or expand access to sexual and reproductive health (273 provisions enacted)
843 provisions introduced that would curtail sexual and reproductive rights or restrict access to sexual and reproductive health (39 provisions enacted)
Abortion
661 provisions introduced that would protect or expand access to abortion care (39 provisions enacted; 7 vetoed)
508 provisions introduced that would restrict access to abortion care (21 provisions enacted; 3 vetoed)
21 provisions introduced that added or expanded existing exceptions to abortion bans (none enacted)
Gender-affirming care
60 provisions introduced that would protect or expand access to gender-affirming care (5 provisions enacted)
80 provisions introduced that would restrict access to gender-affirming care (6 provisions enacted)
Contraception
359 provisions introduced that would protect or expand access to contraceptive services (28 provisions enacted)
Attacks on Sexual and Reproductive Health and Rights
In 2024, policymakers hostile to SRHR continued to target key areas where they were already enforcing bans and restrictions, such as abortion, pregnancy criminalization and gender-affirming care, while also finding new ways to restrict access to essential health services. Twenty-one abortion restrictions were enacted in 2024, many of which increased funding to anti-abortion centers. These interconnected attacks highlight the need for policy that expands and protects access to the full spectrum of SRHR.
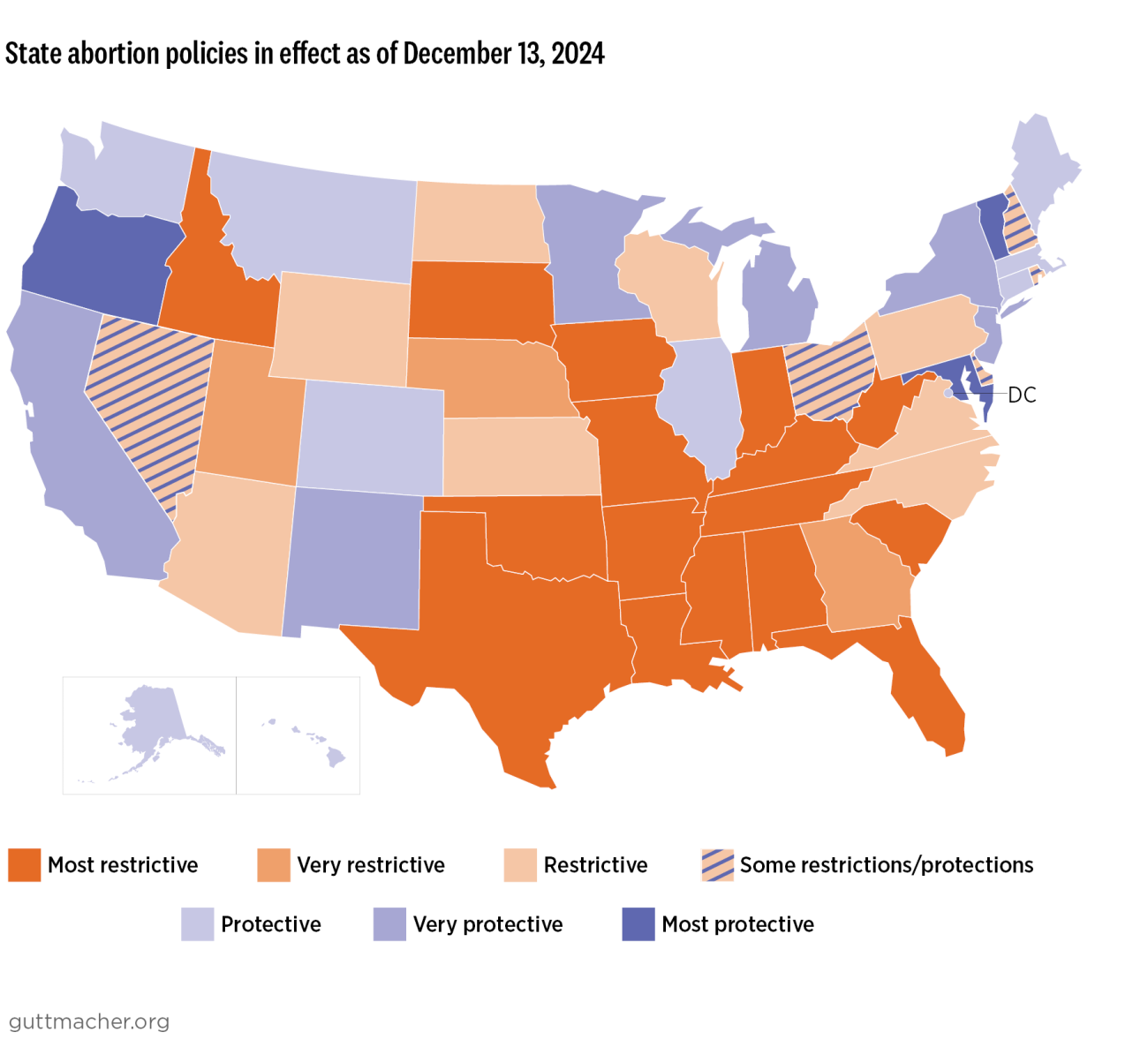
Abortion bans
As of December 13:
- 13 states are enforcing total bans
- 28 states are enforcing abortion bans based on gestational duration
- 7 states currently ban abortion at or before 18 weeks' gestation
- 21 states ban abortion at some point after 18 weeks
Abortion bans in early pregnancy are concentrated in the South, Southeast and Midwest, affecting not just state residents but also creating regional ripple effects. Guttmacher data shows that interstate travel for abortion care doubled from 2020 to 2023. As more states impose bans, people need to travel further for care, which is increasingly difficult for those with limited resources, especially given that donations to abortion funds are dwindling.