
New Guttmacher Institute research from the Monthly Abortion Provision Study shows that there were approximately 642,700 medication abortions in the United States in 2023, accounting for 63% of all abortions in the formal health care system. This is an increase from 2020, when medication abortions accounted for 53% of all abortions.
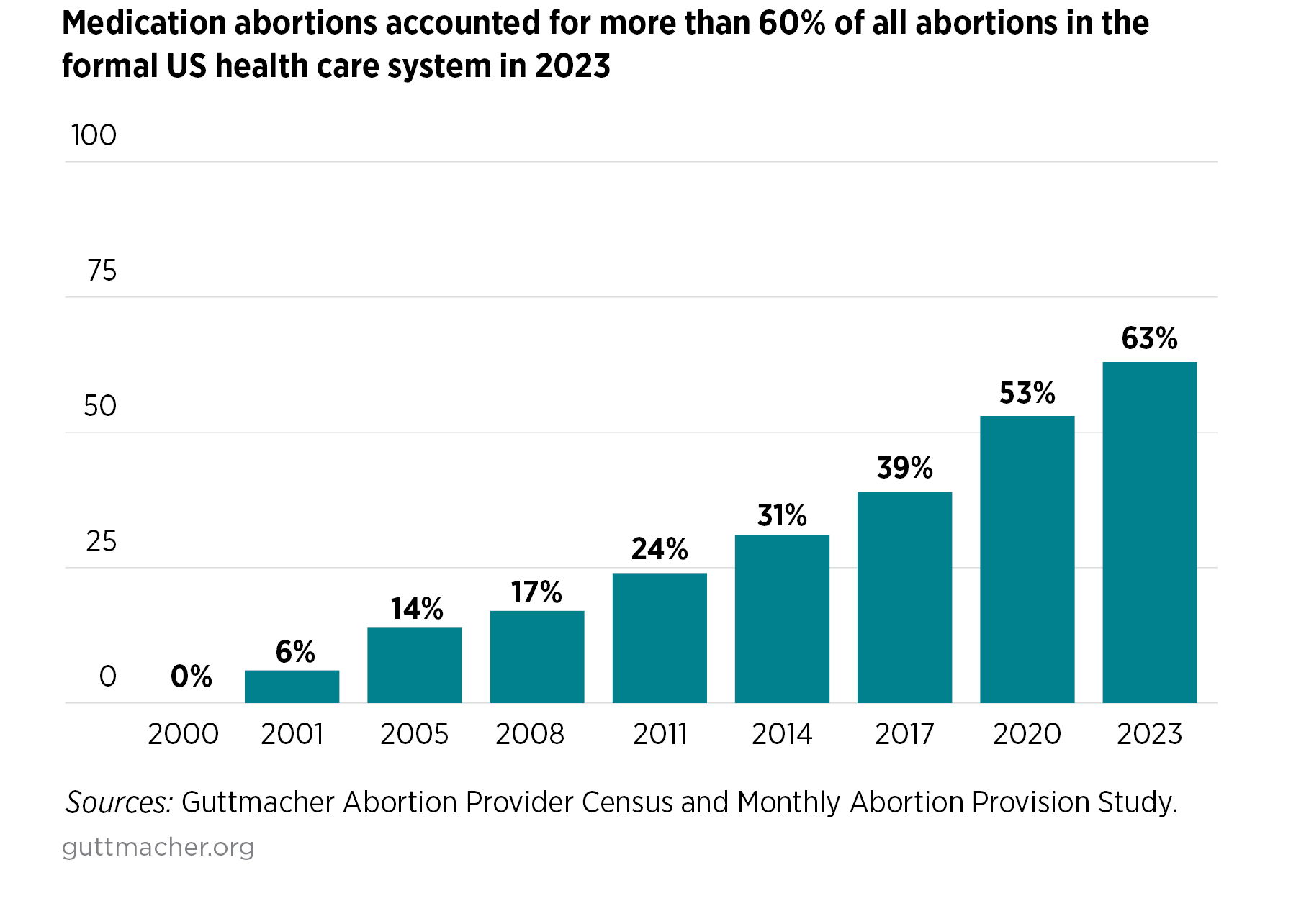
Medication abortion using mifepristone was first approved for use in the United States by the U.S. Food and Drug Administration (FDA) in 2000, and reliance on medication abortion has increased steadily as it has become more accessible over time. The two-drug combination of mifepristone and misoprostol is the most common medication abortion regimen offered by US providers, and decades of research have established that medication abortion using mifepristone is highly safe and effective. Increased access to and use of medication abortion is likely one reason why the overall number of abortions in the formal health care system increased 10% nationally between 2020 and 2023.
The medication abortion counts for 2023 do not include self-managed medication abortions that take place outside of the formal health care system or abortion medication mailed to people in states with total abortion bans. While there are no comprehensive data on the number of self-managed medication abortions in the United States, evidence suggests they have been increasing in the past several years. Therefore, the total count of medication abortions nationally is higher than our count of those offered within the formal health care system.
Unfortunately, gains in access to and use of medication abortion are at risk. The US Supreme Court will hear a case on March 26—Alliance for Hippocratic Medicine v. FDA—that uses low-quality science to challenge access to medication abortion using mifepristone. The Court could restrict the ability to mail mifepristone directly to patients and reinstate the requirement for the drug to be provided in person. If outdated and medically unnecessary restrictions are placed on the provision of mifepristone—in contrast with the FDA’s evidence-based protocol—access to abortion across the country would be greatly impacted.
Medication Abortion Has Become More Widely Available
For many people, medication abortion is more accessible than a procedural abortion. In 2021 (the most recent year with available data), 40% of facilities known to provide abortion care offered only medication abortion. And, starting in 2021, the FDA lifted medically unnecessary restrictions that had required in-person provision of mifepristone. That regulation change, which the FDA finalized in January 2023, meant that health care providers and online pharmacies could mail abortion medication to patients, including those who live far from a provider or are otherwise unable to make an in-person visit. In addition, brick-and-mortar pharmacies can now become certified to dispense and fill mifepristone prescriptions, so access is expected to continue growing.
The number of US providers offering a telemedicine consultation—by video, phone call, text or online platform—and mailing abortion pills increased from 7% of all providers known to offer medication abortion in 2020 to 31% in 2022. Online-only clinics, after first appearing as a new type of abortion provider in 2021, accounted for 8% of all abortions provided within the formal health care system in the first six months of 2023.
Medication abortion provided via telemedicine is as safe and effective as provision in a health care facility. Offering options besides in-person care can reduce, or even remove, some of the secondary costs related to seeking an abortion, such as transportation, child care and missed wages from taking time off work. Like with other types of health care, having the option to access abortion care via telemedicine allows for more flexibility and can expand person-centered care by meeting patients where they want to be served.
Not All People Prefer Medication Abortion Over Procedural Abortion
While broader access to medication abortion has likely contributed to its increased use, it does not necessarily indicate that all people are getting their preferred method.
Since the Supreme Court’s Dobbs v. Jackson Women’s Health Organization decision in June 2022 ended a right to abortion nationally, there has been an increase in patients at clinics in states where abortion continues to be available. Sixteen percent of abortion patients traveled out of state for an abortion in 2023, and there has been increased demand on providers in states that border one of the 14 states where abortion is totally banned. At the same time, abortion has also increased among residents in almost all of these bordering states. In some places, these developments have led to wait times of two weeks or longer for abortion care.
Some individuals may opt to access care through telehealth options to avoid long wait times for appointments, even if they would have preferred in-clinic care. Even at brick-and-mortar clinics, wait times may be shorter for medication abortion than procedural abortion since the pills can be offered by methods such as “quick pick-up.” Finally, for some patients, the closest abortion provider may only offer medication abortion, limiting their access to a procedural abortion unless they can travel to a clinic where it is offered.
When procedural abortion is harder to access relative to medication abortion, the impact of those restricted options falls hardest on groups of people historically marginalized within the health care system. For example, research suggests that Black individuals, people who have had a prior abortion and those with incomes below the federal poverty level are less likely than other groups to prefer, and to have, a medication abortion (vs. a procedural abortion).
State Restrictions on Use of Medication Abortion
Anti-abortion policymakers have been working to restrict access to abortion care on many fronts. Besides the 14 states that are enforcing a total ban on abortion, five states where abortion remains legal until at least six weeks’ gestation have laws that restrict access to medication abortion via telemedicine. Arizona, Nebraska, North Carolina, South Carolina and Wisconsin require that a patient being prescribed medication abortion have an in-person visit with a physician, and Arizona and North Carolina also ban mailing medication abortion pills to a patient. Furthermore, 15 states require medication abortion to be provided by a physician, despite evidence that advanced practice clinicians can provide it safely, as they do in other states.
It Is Critical to Ensure Full Access to Medication Abortion
Medication abortion has proven to be a game changer in expanding abortion care in the United States. Unfortunately, legal attacks and restrictive policies continue to challenge access. When the Supreme Court rules on the case challenging access to mifepristone this spring, it will have to decide whether to ignore the FDA and reimpose unnecessary barriers to access or to respect the scientific evidence that mifepristone is safe and effective.
Any return to restrictions on medication abortion provision via telemedicine would be detrimental for people who either prefer or only have access to abortion using telemedicine. While the current court case only affects use of mifepristone—and a misoprostol-only regimen is also a safe and effective method of medication abortion—everyone seeking an abortion should have access to the full range of safe, effective options.
Methodology
Data on medication abortion for 2023 are from Guttmacher’s Monthly Abortion Provision Study, which produces national and state estimates of the number of abortions provided within the formal health care system in the United States based on data collected from samples of abortion providers. Questions about medication abortion were included in versions of the survey distributed to providers in August and September 2023 and in February 2024 (with the latter asking providers for annual medication abortion figures for 2023). Estimates include abortions provided at brick-and-mortar facilities (including those that use telehealth) and online-only providers. These estimates do not include abortions obtained outside of the formal health care sector or any abortions—whether self-managed or provided by out-of-state clinicians—involving medication mailed to states with total abortion bans.
